
Treatment Guidelines
Treatment Approaches for Eosinophilic Esophagitis
Stanislaw J. Gabryszewski, MD, PhD; Claire A. Beveridge, MD; Corey J. Ketchem, MD, MSCE; Simin Zhang, MD; Girish Hiremath, MD, MPH
This review focuses on currently accepted therapies for eosinophilic esophagitis (EoE), the most well-studied of the eosinophilic gastrointestinal disorders (EGIDs), for which the most robust evidence and clinical guidelines exist. In the case of non-EoE EGIDs—including eosinophilic gastritis (EoG), eosinophilic enteritis (EoN), and eosinophilic colitis (EoC)—the relative rarity and heterogeneity of these diseases have limited the development of standardized treatment guidelines. Recent European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) / North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) guidelines for pediatric non-EoE EGIDs represent an important step forward and shed light on the potential for expanded, evidence-based guidance as the EGID field evolves.1 One of the driving forces behind the creation of the Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR) is to increase the number of patients studied to support the development of evidence-based treatment protocols for all EGIDs.
Introduction
Introduction
EoE is an allergen-mediated disease of the esophagus that affects people of all ages worldwide.2 Histologically, it is characterized by an eosinophil-predominant inflammation [defined as peak eosinophil count (PEC) of ≥ 15 eosinophils per high-power field] in the esophagus.3 Given its chronic and progressive course, affected individuals present with age-dependent esophageal symptoms. For instance, children commonly present with vomiting, feeding difficulties, and abdominal pain.4, 5 A delay in diagnosis or uncontrolled eosinophilic inflammation in the esophageal epithelium can be associated with suboptimal quality of life and lead to fibrostenotic complications, such as esophageal narrowing or stricture, resulting in esophageal food impaction (EFI).6, 7 Therefore, resolution of clinical symptoms and histologic remission (defined as a decrease in PEC to < 15 eosinophils per high-power field with mucosal healing) are among the primary goals of treating EoE.
Over the past three decades, our understanding of EoE has substantially improved. Once considered a rare and case-reportable disease,8 EoE has emerged as a well-characterized, clinicopathologic condition and one of the more heavily researched upper gastrointestinal diseases. Emerging evidence suggests that type 2 helper T (Th2) cell‒driven inflammation involving T cells, eosinophils, mast cells, and cytokines, such as interleukin (IL)-4, IL-5, thymic stromal lymphopoietin (TSLP), and IL-13, is fundamental to the immunopathogenesis of EoE.9, 10 In addition, genome-wide association studies have identified multiple genes, such as TSLP and STAT6, that play roles in Th2 cell differentiation and development, as well as genes that are vital to epithelial cell function and esophageal epithelial barrier integrity.11 Growth of our knowledge base has led to the evolution of diagnostic and management guidelines from an expert opinion or consensus statement to an evidence-based approach.12-16 It has also spurred a host of treatments and has raised the possibility of personalizing EoE therapies.
The currently accepted EoE therapies are collectively referred to as the “3 D’s”: dietary elimination, drugs [e.g., proton pump inhibitors (PPI), topical corticosteroids (TCS), and biologics], and esophageal dilation (Figure). Shared decision-making is a key component of managing EoE, with the goal of inducing and maintaining remission to minimize the risk of fibrostenotic complications. Choosing which approach to pursue is typically based on the shared decision-making between the patient, caregivers, and healthcare providers.17 Endoscopic interventions, such as esophageal dilation, are generally considered for patients with complicated EoE.18
Dietary Elimination
The rationale for dietary intervention is to control eosinophilic inflammation by eliminating food allergens presumed to cause EoE and avoiding medications and their associated side effects.19 At present, elemental diet and empiric elimination diets are the hallmark dietary strategies. Allergy test‒directed elimination is a historical approach that has fallen out of favor due to poor accuracy.15
An elemental diet is an allergen-free diet that uses amino acid‒based formulas as the sole source of nutrition. In the context of EoE, an elemental diet is about 91% effective in controlling esophageal eosinophilic inflammation, although it has significant limitations, including high cost, palatability issues, a long reintroduction period, and frequent endoscopy (EGD) with biopsies to identify the food allergen.20–22
An empiric elimination diet is a more well-studied dietary management approach for EoE. It involves the elimination of foods, including dairy, egg, wheat, soy, nuts (including peanuts and tree nuts), and seafood (including fish and shellfish), which are food allergens commonly associated with EoE.15, 23 In clinical practice, most patients have 1-3 food triggers. There are several ways to implement the empiric elimination diet.24, 25 Options include one-food elimination (1FED, usually dairy with up to 68% cumulative efficacy), two-food elimination (2FED, usually dairy and wheat with 43% cumulative efficacy), four-food elimination (4FED, usually dairy, wheat, egg, soy with up to 71% cumulative efficacy), and six-food elimination (6FED with incremental efficacy of up to 78% cumulative efficacy).26 Furthermore, one can employ an empiric elimination diet as a step-up (1FED, 2FED, 4FED, and 6FED) or a step-down (6FED, 4FED, 2FED, and 1FED) approach in clinical practice.27 Once again, choosing which approach to pursue is typically based on shared decision-making between the patient, caregivers, and healthcare providers. CEGIR conducted a multi-site, randomized, prospective trial comparing 1FED (milk elimination) vs. 6FED (milk, wheat, egg, soy, nuts, fish elimination).28 Interestingly, this study showed similar responses between 1FED and 6FED, both achieving remission rates of approximately 40%. These findings provide a strong rationale for first starting with dairy elimination therapy.
Current guidelines do not recommend allergy test‒directed elimination diets for EoE management, as the predictive accuracy of current allergy testing is limited in identifying EoE triggers.15 An allergy test‒directed elimination diet is based on eliminating food allergens and aeroallergens, as identified by serum specific IgE, skin prick testing, or in some cases atopy patch testing. These tests are used to evaluate allergic disease, and food allergy testing is particularly helpful in the diagnosis of IgE-mediated food allergy, which may co-occur with EoE. Among EoE patients, milk, egg, wheat, and soy are among the most common food allergens identified through allergy tests in children, whereas peanut, egg, and soy are among the most common food allergens identified through allergy tests in adults.29-31 However, a meta-analysis of 33 studies (including 1,317 individuals with EoE) reported a 45.5% success rate for allergy test‒based elimination diets, making this the least effective dietary elimination strategy.
Pursuing a dietary elimination approach to identify triggering food allergens can be expensive, time-consuming, and often requires multiple endoscopies with biopsies to confirm treatment response or relapse of EoE. It may also be associated with growth issues and nutritional deficiencies, particularly in children.32 Furthermore, it can have unintended ramifications for the patients' and their caregivers' social and emotional well-being.33 These considerations should be discussed with patients and their families as treatment options are being compared.
Medications
Proton Pump Inhibitors
Many consider PPIs as first-line therapy because this medication has been used for a long time for non-EoE indications. Additionally, PPIs are well-studied in EoE, readily available, and relatively easy to administer. PPIs can be administered as a tablet or capsule. For those who have difficulty swallowing a tablet, they can be administered as oral solution, orodispersible tablet, or granules (opened capsule) that can be mixed with applesauce. It is now appreciated that the mechanism of PPI therapy in EoE is not only related to acid suppression‒related protection of the esophageal epithelial barrier, but also to direct anti-inflammatory effects. Once administered, PPIs induce gastric acid suppression, inhibit eosinophilic migration to the esophagus, inhibit ATP12A, activate the aryl hydrocarbon receptor, and reduce STAT6-mediated expression of eotaxin-3 (an eosinophil chemoattractant), thus leading to the resolution of eosinophilic inflammation and restoration of esophageal barrier function.34-36 The histologic response rate for PPI therapy is approximately 50%.36, 37 For children with EoE, the current recommendation is 1-2 mg per kg of body weight per day, divided twice daily, with a maximum of 40 mg twice daily of esomeprazole and omeprazole and 30 mg twice daily of lansoprazole. For adults with EoE, the recommended dose is 20-40 mg once or twice daily for esomeprazole and omeprazole and 30 mg once or twice daily for lansoprazole. EGD with biopsies is recommended between 8 and 12 weeks to assess the treatment response.12, 15, 38
The American Gastroenterological Association Joint Task Force EoE management guidelines and American College of Gastroenterology clinical guidelines recommend PPI therapy for patients with symptomatic esophageal eosinophilia, but this is a conditional recommendation with limited high-quality evidence.15 The available evidence is limited by the lack of placebo-controlled studies and heterogeneity in study design (i.e., patient selection and type, dose, and duration of PPIs). In general, ‘high-dose’ PPI is recommended, and it is reasonable to try to wean down to the lowest most effective dose.15 There are limited data on the efficacy of PPIs as a maintenance therapy for EoE.13 Up to 78% of patients maintain remission at a 1-year follow up.39, 40 In terms of potential risks of PPIs, a randomized control trial in 2019 showed no increased risk of osteopenia, osteoporosis, dementia, and renal disease.36, 41
Topical Corticosteroids
Mechanistically, TCS alleviates eosinophilic inflammation in the esophageal epithelium, lowers epithelial cell apoptosis, decreases esophageal molecular remodeling, reduces the dilated intercellular spaces, and downregulates mast cell activity.42 The two most used TCS in clinical practice are budesonide43-47 and fluticasone propionate.48-50
Budesonide is commonly administered as a slurry [oral viscous Budesonide (OVB)] mixed with various ‘vehicles’, including sucralose, Neocate Nutra (a semi-solid, amino acid-based hypoallergenic formula), honey, and apple sauce.51 Mixing with a vehicle of the patient’s choice allows for optimal consistency, adequate contact time with the esophageal mucosa, and palatability that can promote compliance with the medication.52 The FDA has approved budesonide oral suspension (BOS) for those 11 years old and over at 2 mg twice a day for 12 weeks.45, 53 Budesonide is also approved as orodispersible tablets in Europe.47, 54, 55
Fluticasone propionate can be delivered via a metered-dose inhaler (MDI), a diskus (a device containing medication in blister packs), or an oral viscous suspension. The most common route of administration for fluticasone is via MDI. The patient directly sprays medication into their mouth (without a spacer) and then swallows it. They then rinse their mouths and spit to avoid oral side effects. A video demonstration of this technique is available here. Although some retrospective studies have suggested that treatment with OVB leads to better endoscopic and histologic outcomes than fluticasone propionate,56, 57 prospective randomized clinical trials have shown that both OVB and fluticasone MDI produced a comparable significant improvement in dysphagia and endoscopic features and a decrease in esophageal eosinophilia.58 Other TCS, although less commonly used, are ciclesonide59-61, mometasone,62 and beclomethasone.63, 64 Possible adverse effects of TCS include esophageal candidiasis and adrenal axis suppression, including concerns for suppression of height velocity.65, 66 Though systemic steroids (prednisone)50 have been used infrequently in clinical practice, they are not considered as the mainstay of EoE treatment due to their established side effect profile.
Biologics
Biologics are therapeutic agents, typically monoclonal antibodies or recombinant proteins, designed to selectively target specific components of the immune system involved in disease pathogenesis. With a greater understanding of the molecular mechanisms underlying EoE, limitations of conventional therapies, and advances in targeted immunomodulation, biologic therapies have emerged as a promising treatment strategy.67
Anti‒IL-4/IL-13 Pathway
Targeting upstream Th2 cytokines has yielded the most clinically meaningful results to date. Dupilumab, a monoclonal antibody directed against the IL-4 receptor α subunit, inhibits signaling by both IL-4 and IL-13, key cytokines that drive inflammation and remodeling in EoE.68 In a pivotal phase 3 randomized, placebo-controlled trial, dupilumab administered subcutaneously at a weekly dose of 300 mg achieved significant improvements in both histologic remission and dysphagia symptoms compared with placebo.69 The histologic improvement with the every-two-week dosing regimen was qualitatively similar to that with the weekly dosing regimen. However, the differences between every two-week regimen and the placebo did not achieve statistical significance. These findings led to FDA approval in 2022, making dupilumab the first approved biologic therapy for EoE. Subsequent studies have demonstrated consistent efficacy across pediatric and adolescent populations.70 Injection-site reaction (most common), upper respiratory infections, arthralgia, and conjunctivitis were among the adverse events reported.69 Dupilumab is a compelling treatment option, in particular for those who have had an inadequate response to, or are intolerant of, conventional therapies and/or concurrent atopic comorbidities (e.g., eczema and/or asthma).
Anti‒IL-5 Pathway
The first biologics studied in EoE targeted IL-5, a key regulator of eosinophil differentiation, recruitment, and survival. Mepolizumab and reslizumab demonstrated reductions in esophageal eosinophil counts and improvement in histologic measures in randomized trials.71-77 However, these histologic gains did not translate into meaningful improvements in patient-reported symptoms or quality of life. Similarly, benralizumab, which targets the IL-5Rα chain and induces eosinophil depletion, resulted in histologic remission but showed limited and inconsistent symptomatic benefit.78 The discordance between histologic response and symptom improvement has been a key insight from these studies, suggesting that eosinophils alone may not fully account for disease manifestations. Other contributors, including mast cells, fibrosis, and neurosensory dysfunction, likely play important roles in symptom generation.79 Consequently, anti‒IL-5 therapies have not demonstrated sufficient clinical efficacy to support routine use in EoE and remain unapproved for this indication.
Anti-IgE
Omalizumab, an anti-IgE monoclonal antibody, was initially explored given the atopic associations of EoE.80 However, randomized studies have failed to demonstrate significant histologic or symptomatic improvement compared with placebo, suggesting that IgE is not a primary driver of the disease in most patients.81
Anti‒IL-13 Pathway
Selective IL-13 inhibition has emerged as another promising strategy given IL-13’s role in epithelial barrier dysfunction and tissue remodeling.82 Cendakimab, an IL-13‒targeting monoclonal antibody, has demonstrated significant reductions in esophageal eosinophilia along with improvements in endoscopic and symptomatic outcomes in phase 2 and phase 3 trials.83, 84 Though these results are encouraging, regulatory approval is pending, and the role of this therapy in clinical practice remains under investigation.
Anti-Siglec-8
Lirentelimab (AK002), a Siglec-8‒targeting monoclonal antibody, induces apoptosis of eosinophils and inhibits mast cells.85, 86 In phase 2/3 trials, lirentelimab achieved significant histologic improvement but failed to meet primary symptom endpoints, although trends toward improvement were observed in some subgroups.87
Anti-TSLP
There is increasing interest in targeted interruption of upstream inflammatory pathways, including inhibition of TSLP. A phase 3 trial to investigate the efficacy and safety of the anti-TSLP biologic tezepelumab in EoE is currently underway (NCT05583227). Solriktug is another investigational monoclonal antibody targeting TSLP, and it is being studied in a phase 2 trial in adults with EoE (NCT06598462).
Other Biologics
Tumor necrosis factor α inhibitors (e.g., infliximab)88 and anti-integrin therapies (e.g., vedolizumab)89-91 have been studied in small cohorts or case series with limited success, requiring further research to understand their potential therapeutic benefit. Etrasimod, a sphingosine-1-phosphate (S1P) receptor modulator, represents a mechanistically distinct approach by modulating lymphocyte trafficking rather than directly targeting cytokines. Early-phase studies demonstrate reductions in eosinophil counts and improvements in histologic and symptomatic measures, though larger trials are needed to define its clinical potential.92
Clinical Considerations and Future Directions for Biologics
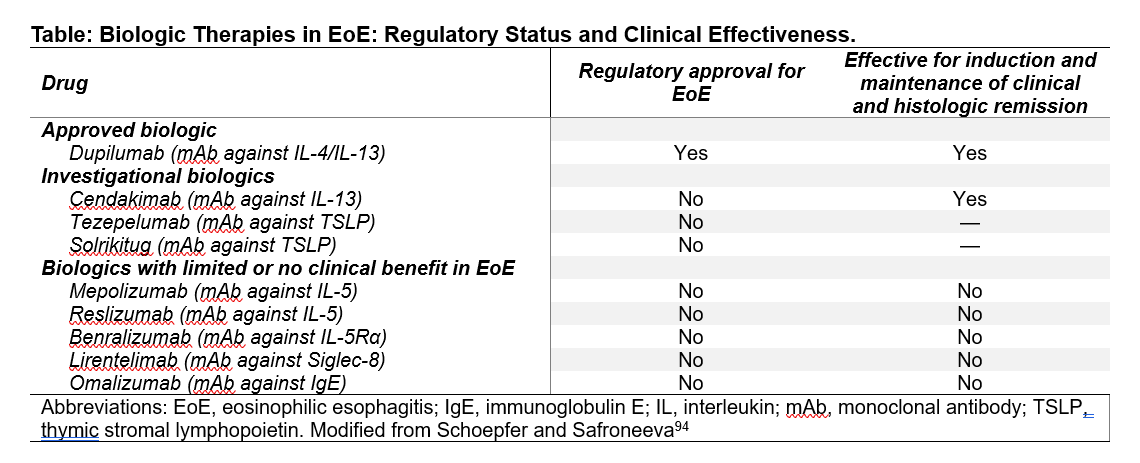
The expanding biologic landscape highlights the complexity of EoE pathophysiology and highlights the need for therapies that address both inflammation and remodeling (Table). However, several factors, including cost, accessibility, effectiveness, safety, and the duration of clinical and histologic response, will influence the positioning of biologics in the therapeutic algorithm.93 Key unanswered questions include optimal treatment sequencing, patient selection, long-term safety, and the ability of biologics to prevent or reverse fibrostenotic remodeling. As additional agents emerge, comparative effectiveness studies and individualized approaches will be important to guide therapy.
Dilation
Repeated EGD with biopsies remains essential for the diagnosis and monitoring of EoE and also serves a critical therapeutic role in the management of fibrostenotic complications, including esophageal strictures and EFIs. Esophageal dilation is a cornerstone intervention for the sequelae of fibrosis resulting from chronic inflammation and remodeling.15, 95 Additionally, prior observational work has demonstrated increasing rates of esophageal stricture formation and dilation over the past two decades, reflecting the growing burden of fibrostenotic disease in EoE and reinforcing the importance of this intervention.96
Esophageal stricturing can be focal or more diffuse (narrow-caliber esophagus). The target esophageal caliber is considered 16-18 mm in adolescents and adults and has been associated with symptomatic improvement and a reduced risk of food impaction. Though a single dilation is generally safe and effective,97 many patients require serial dilations to achieve and maintain this luminal diameter. Importantly, dilation addresses the mechanical consequences of fibrosis but does not treat the underlying eosinophilic inflammation, necessitating concomitant medical or dietary therapy to reduce recurrence and future dilation requirements.15
Endoscopic dilation techniques have evolved and are generally well tolerated. Through-the-scope balloon dilators are commonly used, particularly for focal strictures.98-100 Dilation with Savary and Maloney bougies is also employed and is particularly useful for proximal and multifocal strictures. Technique selection largely depends on endoscopists' experience and preference, with limited evidence supporting the superiority of one over another.98
EFI is relatively common in adolescents and adults with EoE. It can be the presenting symptom of EoE in up to 55% of patients, and a quarter of patients have recurrent food impactions.101, 102 Management typically requires urgent EGD for food bolus removal, using a variety of techniques (e.g., en bloc, piecemeal, cap-assisted, or push techniques) and tools such as forceps, snares, retrieval nets, or baskets.103-106 More than one tool and technique may be required in complex cases. Following disimpaction, obtaining esophageal biopsies away from the impaction site is strongly recommended, given the high association with EoE and the need for histologic confirmation.53, 107 Mucosal friability related to active inflammation and esophageal remodeling may place individuals with EFI at increased risk of perforation and bleeding during removal of an impacted food bolus or dilation of esophageal strictures.108 Typically, these complications are managed conservatively. No deaths have been reported related to either esophageal perforation or therapy.109
Overall, though esophageal dilation is a safe and effective therapy for fibrostenotic disease in EoE, key gaps remain in defining optimal, evidence-based dilation strategies. Addressing these uncertainties, particularly regarding longitudinal outcomes and optimal procedural approaches, represents an important opportunity to guide data-driven dilation practices.
Towards Precision Medicine: Leveraging Multimodal Data and Artificial Intelligence
As the molecular and clinical heterogeneity of EoE becomes better defined, there is growing interest in precision medicine approaches, including those augmented by artificial intelligence (AI), to better characterize disease subtypes and inform management. Emerging applications, such as digital histopathology, multimodal integration, and longitudinal modeling of disease trajectories, offer the potential to enhance disease characterization and predict treatment response. However, challenges, including heterogeneity of data sources, small patient cohorts, and limited generalizability, have thus far limited the translation of these approaches into clinical practice.110-112
To date, a number of investigational insights have heightened interest in developing precision medicine approaches. For example, transcriptomic analyses have identified distinct EoE endotypes, including those with prominent eosinophilic inflammation and fibrostenotic remodeling.113 In addition, pharmacogenomic studies suggest that variability in treatment response may be, in part, explained by host genetic factors. For example, PPI non-response may be related to subtherapeutic drug exposure in patients with CYP2C19 rapid-metabolizer variants, and polymorphisms in STAT6 (e.g., rs324011) have been associated with an increased risk of incomplete remission or disease relapse.114, 115 Continued biomarker discoveries may further shape the precision medicine landscape. For example, esophageal microRNA profiles can distinguish PPI responders from nonresponders at baseline,116 and immune signatures (e.g., food-specific IgG4) have been correlated with response to dietary therapy.117 In parallel, there is increasing interest in developing non-invasive biomarkers and minimally invasive techniques to monitor disease activity and treatment response over time.15 Collectively, these advances illustrate an evolving framework for precision medicine in EoE, with the hope of transforming EoE diagnosis and treatment as evidence and understanding continue to grow.
Conclusion
EoE is an increasingly prevalent, chronic, and progressive disease affecting all ages worldwide. Dietary elimination of food allergens, pharmacotherapy, and esophageal dilation are the current mainstays of treatment. As the molecular and clinical heterogeneity of EoE continues to be unraveled, novel targeted therapies may further expand EoE treatment options. Relatedly, there is growing interest in transitioning from a “one-size-fits-all” approach to an AI-guided precision medicine approach, wherein the phenotype and the endotype of a patient with EoE will be used to guide the patient's treatment. These principles will ideally extend to the rarer, non-EoE EGIDs as additional data emerge and evidence and understanding continue to expand.
Figure
Figure: Schematic of Treatment Approaches for EoE. Currently accepted therapies for EoE fall into three major categories (i.e., the “3 D’s”): dietary elimination, drugs (i.e., proton pump inhibitors, topical corticosteroids, and biologics), and esophageal dilation for complicated disease. Shared decision-making is a key component in determining the best approach for a given patient.
Acknowledgements
The authors thank Shawna Hottinger, a medical writer employed by Cincinnati Children’s Hospital Medical Center, for editorial assistance.
References
- Papadopoulou A, Amil-Dias J, Auth MK, Chehade M, Collins MH, Gupta SK, Gutierrez-Junquera C, Orel R, Vieira MC, Zevit N, Atkins D, Bredenoord AJ, Carneiro F, Dellon ES, Gonsalves N, Menard-Katcher C, Koletzko S, Liacouras C, Marderfeld L, Oliva S, Ohtsuka Y, Rothenberg ME, Strauman A, Thapar N, Yang GY, Furuta GT. Joint ESPGHAN/NASPGHAN Guidelines on Childhood Eosinophilic Gastrointestinal Disorders Beyond Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr. 2024;78(1):122-52. Epub 20230704. doi: 10.1097/MPG.0000000000003877. PubMed PMID: 38291684.
- Navarro P, Arias A, Arias-Gonzalez L, Laserna-Mendieta EJ, Ruiz-Ponce M, Lucendo AJ. Systematic review with meta-analysis: the growing incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment Pharmacol Ther. 2019;49(9):1116-25. Epub 20190318. doi: 10.1111/apt.15231. PubMed PMID: 30887555.
- Furuta GT, Katzka DA. Eosinophilic Esophagitis. N Engl J Med. 2015;373(17):1640-8. doi: 10.1056/NEJMra1502863. PubMed PMID: 26488694; PMCID: PMC4905697.
- Hiremath G, Rogers E, Kennedy E, Hemler J, Acra S. A Comparative Analysis of Eating Behavior of School-Aged Children with Eosinophilic Esophagitis and Their Caregivers' Quality of Life: Perspectives of Caregivers. Dysphagia. 2019;34(4):567-74. Epub 20190202. doi: 10.1007/s00455-019-09984-x. PubMed PMID: 30712065; PMCID: PMC6660376.
- Straumann A, Aceves SS, Blanchard C, Collins MH, Furuta GT, Hirano I, Schoepfer AM, Simon D, Simon HU. Pediatric and adult eosinophilic esophagitis: similarities and differences. Allergy. 2012;67(4):477-90. Epub 20120208. doi: 10.1111/j.1398-9995.2012.02787.x. PubMed PMID: 22313241.
- Dellon ES, Kim HP, Sperry SL, Rybnicek DA, Woosley JT, Shaheen NJ. A phenotypic analysis shows that eosinophilic esophagitis is a progressive fibrostenotic disease. Gastrointest Endosc. 2014;79(4):577-85 e4. Epub 20131123. doi: 10.1016/j.gie.2013.10.027. PubMed PMID: 24275329; PMCID: PMC4599711.
- Schoepfer AM, Safroneeva E, Bussmann C, Kuchen T, Portmann S, Simon HU, Straumann A. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013;145(6):1230-6 e1-2. Epub 20130813. doi: 10.1053/j.gastro.2013.08.015. PubMed PMID: 23954315.
- Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology. 1995;109(5):1503-12. doi: 10.1016/0016-5085(95)90637-1. PubMed PMID: 7557132.
- Blanchard C, Wang N, Rothenberg ME. Eosinophilic esophagitis: pathogenesis, genetics, and therapy. J Allergy Clin Immunol. 2006;118(5):1054-9. Epub 20060918. doi: 10.1016/j.jaci.2006.07.038. PubMed PMID: 17088129.
- Ryu S, Lee KH, Tizaoui K, Terrazzino S, Cargnin S, Effenberger M, Shin JI, Kronbichler A. Pathogenesis of Eosinophilic Esophagitis: A Comprehensive Review of the Genetic and Molecular Aspects. Int J Mol Sci. 2020;21(19). Epub 20200930. doi: 10.3390/ijms21197253. PubMed PMID: 33008138; PMCID: PMC7582808.
- Sleiman PM, Wang ML, Cianferoni A, Aceves S, Gonsalves N, Nadeau K, Bredenoord AJ, Furuta GT, Spergel JM, Hakonarson H. GWAS identifies four novel eosinophilic esophagitis loci. Nat Commun. 2014;5:5593. Epub 20141119. doi: 10.1038/ncomms6593. PubMed PMID: 25407941; PMCID: PMC4238044.
- Lucendo AJ, Molina-Infante J, Arias A, von Arnim U, Bredenoord AJ, Bussmann C, Amil Dias J, Bove M, Gonzalez-Cervera J, Larsson H, Miehlke S, Papadopoulou A, Rodriguez-Sanchez J, Ravelli A, Ronkainen J, Santander C, Schoepfer AM, Storr MA, Terreehorst I, Straumann A, Attwood SE. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J. 2017;5(3):335-58. Epub 20170123. doi: 10.1177/2050640616689525. PubMed PMID: 28507746; PMCID: PMC5415218.
- Hirano I, Chan ES, Rank MA, Sharaf RN, Stollman NH, Stukus DR, Wang K, Greenhawt M, Falck-Ytter YT, Committee AGAICG, Joint Task Force on Allergy-Immunology Practice P. AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters Clinical Guidelines for the Management of Eosinophilic Esophagitis. Gastroenterology. 2020;158(6):1776-86. doi: 10.1053/j.gastro.2020.02.038. PubMed PMID: 32359562; PMCID: PMC9473154.
- Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon ES, Dohil R, Falk GW, Gonsalves N, Gupta SK, Katzka DA, Lucendo AJ, Markowitz JE, Noel RJ, Odze RD, Putnam PE, Richter JE, Romero Y, Ruchelli E, Sampson HA, Schoepfer A, Shaheen NJ, Sicherer SH, Spechler S, Spergel JM, Straumann A, Wershil BK, Rothenberg ME, Aceves SS. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128(1):3-20 e6; quiz 1-2. Epub 20110407. doi: 10.1016/j.jaci.2011.02.040. PubMed PMID: 21477849.
- Dellon ES, Muir AB, Katzka DA, Shah SC, Sauer BG, Aceves SS, Furuta GT, Gonsalves N, Hirano I. ACG Clinical Guideline: Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2025;120(1):31-59. Epub 20250102. doi: 10.14309/ajg.0000000000003194. PubMed PMID: 39745304.
- Furuta GT, Liacouras CA, Collins MH, Gupta SK, Justinich C, Putnam PE, Bonis P, Hassall E, Straumann A, Rothenberg ME, First International Gastrointestinal Eosinophil Research Symposium S. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007;133(4):1342-63. Epub 20070808. doi: 10.1053/j.gastro.2007.08.017. PubMed PMID: 17919504.
- Sauer BG, West A, McGowan EC. Multidisciplinary Eosinophilic Esophagitis Care: A Model for Comprehensive Patient-Centered Care Through Shared Decision Making Between Gastroenterology, Allergy, and Nutrition. Clin Gastroenterol Hepatol. 2021;19(11):2226-9. Epub 20210716. doi: 10.1016/j.cgh.2021.07.025. PubMed PMID: 34280551.
- Lucendo AJ, Arias A, Molina-Infante J, Arias-Gonzalez L. The role of endoscopy in eosinophilic esophagitis: from diagnosis to therapy. Expert Rev Gastroenterol Hepatol. 2017;11(12):1135-49. Epub 20170817. doi: 10.1080/17474124.2017.1367664. PubMed PMID: 28803528.
- Visaggi P, Mariani L, Pardi V, Rosi EM, Pugno C, Bellini M, Zingone F, Ghisa M, Marabotto E, Giannini EG, Savarino V, Marchi S, Savarino EV, de Bortoli N. Dietary Management of Eosinophilic Esophagitis: Tailoring the Approach. Nutrients. 2021;13(5). Epub 20210512. doi: 10.3390/nu13051630. PubMed PMID: 34066243; PMCID: PMC8151361.
- Peterson KA, Byrne KR, Vinson LA, Ying J, Boynton KK, Fang JC, Gleich GJ, Adler DG, Clayton F. Elemental diet induces histologic response in adult eosinophilic esophagitis. Am J Gastroenterol. 2013;108(5):759-66. Epub 20130205. doi: 10.1038/ajg.2012.468. PubMed PMID: 23381017.
- Markowitz JE, Spergel JM, Ruchelli E, Liacouras CA. Elemental diet is an effective treatment for eosinophilic esophagitis in children and adolescents. Am J Gastroenterol. 2003;98(4):777-82. doi: 10.1111/j.1572-0241.2003.07390.x. PubMed PMID: 12738455.
- Kliewer KL, Cassin AM, Venter C. Dietary Therapy for Eosinophilic Esophagitis: Elimination and Reintroduction. Clin Rev Allergy Immunol. 2018;55(1):70-87. doi: 10.1007/s12016-017-8660-1. PubMed PMID: 29238902.
- Shah M, Sapkota A, Aravindaksha I, Amdetsion GY, Katwal K, Almoghrabi A. Eosinophilic esophagitis and its association with food allergies: A United States national analysis 2016 to 2022. PLoS One. 2025;20(10):e0335078. Epub 20251023. doi: 10.1371/journal.pone.0335078. PubMed PMID: 41129525; PMCID: PMC12548918.
- Lucendo AJ, Arias A, Gonzalez-Cervera J, Yague-Compadre JL, Guagnozzi D, Angueira T, Jimenez-Contreras S, Gonzalez-Castillo S, Rodriguez-Domingez B, De Rezende LC, Tenias JM. Empiric 6-food elimination diet induced and maintained prolonged remission in patients with adult eosinophilic esophagitis: a prospective study on the food cause of the disease. J Allergy Clin Immunol. 2013;131(3):797-804. Epub 20130131. doi: 10.1016/j.jaci.2012.12.664. PubMed PMID: 23375693.
- Kagalwalla AF, Shah A, Li BU, Sentongo TA, Ritz S, Manuel-Rubio M, Jacques K, Wang D, Melin-Aldana H, Nelson SP. Identification of specific foods responsible for inflammation in children with eosinophilic esophagitis successfully treated with empiric elimination diet. J Pediatr Gastroenterol Nutr. 2011;53(2):145-9. doi: 10.1097/MPG.0b013e31821cf503. PubMed PMID: 21788754.
- Arias A, Gonzalez-Cervera J, Tenias JM, Lucendo AJ. Efficacy of dietary interventions for inducing histologic remission in patients with eosinophilic esophagitis: a systematic review and meta-analysis. Gastroenterology. 2014;146(7):1639-48. Epub 20140215. doi: 10.1053/j.gastro.2014.02.006. PubMed PMID: 24534634.
- Molina-Infante J, Arias A, Alcedo J, Garcia-Romero R, Casabona-Frances S, Prieto-Garcia A, Modolell I, Gonzalez-Cordero PL, Perez-Martinez I, Martin-Lorente JL, Guarner-Argente C, Masiques ML, Vila-Miravet V, Garcia-Puig R, Savarino E, Sanchez-Vegazo CT, Santander C, Lucendo AJ. Step-up empiric elimination diet for pediatric and adult eosinophilic esophagitis: The 2-4-6 study. J Allergy Clin Immunol. 2018;141(4):1365-72. Epub 20171023. doi: 10.1016/j.jaci.2017.08.038. PubMed PMID: 29074457.
- Kliewer KL, Gonsalves N, Dellon ES, Katzka DA, Abonia JP, Aceves SS, Arva NC, Besse JA, Bonis PA, Caldwell JM, Capocelli KE, Chehade M, Cianferoni A, Collins MH, Falk GW, Gupta SK, Hirano I, Krischer JP, Leung J, Martin LJ, Menard-Katcher P, Mukkada VA, Peterson KA, Shoda T, Rudman Spergel AK, Spergel JM, Yang GY, Zhang X, Furuta GT, Rothenberg ME. One-food versus six-food elimination diet therapy for the treatment of eosinophilic oesophagitis: a multicentre, randomised, open-label trial. Lancet Gastroenterol Hepatol. 2023;8(5):408-21. Epub 20230228. doi: 10.1016/S2468-1253(23)00012-2. PubMed PMID: 36863390; PMCID: PMC10102869.
- Spergel JM, Beausoleil JL, Mascarenhas M, Liacouras CA. The use of skin prick tests and patch tests to identify causative foods in eosinophilic esophagitis. J Allergy Clin Immunol. 2002;109(2):363-8. doi: 10.1067/mai.2002.121458. PubMed PMID: 11842310.
- Molina-Infante J, Martin-Noguerol E, Alvarado-Arenas M, Porcel-Carreno SL, Jimenez-Timon S, Hernandez-Arbeiza FJ. Selective elimination diet based on skin testing has suboptimal efficacy for adult eosinophilic esophagitis. J Allergy Clin Immunol. 2012;130(5):1200-2. Epub 20120803. doi: 10.1016/j.jaci.2012.06.027. PubMed PMID: 22867695.
- Spergel JM, Andrews T, Brown-Whitehorn TF, Beausoleil JL, Liacouras CA. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann Allergy Asthma Immunol. 2005;95(4):336-43. doi: 10.1016/S1081-1206(10)61151-9. PubMed PMID: 16279563.
- Bashaw H, Schwartz S, Kagalwalla AF, Wechsler JB. Tutorial: Nutrition Therapy in Eosinophilic Esophagitis-Outcomes and Deficiencies. JPEN J Parenter Enteral Nutr. 2020;44(4):600-9. Epub 20191119. doi: 10.1002/jpen.1738. PubMed PMID: 31743470.
- Hiremath G, Kodroff E, Strobel MJ, Scott M, Book W, Reidy C, Kyle S, Mack D, Sable K, Abonia P, Spergel J, Gupta SK, Furuta TG, Rothenberg ME, Dellon ES. Individuals affected by eosinophilic gastrointestinal disorders have complex unmet needs and frequently experience unique barriers to care. Clin Res Hepatol Gastroenterol. 2018;42(5):483-93. Epub 20180331. doi: 10.1016/j.clinre.2018.03.003. PubMed PMID: 29615329; PMCID: PMC6167209.
- Cheng E, Zhang X, Huo X, Yu C, Zhang Q, Wang DH, Spechler SJ, Souza RF. Omeprazole blocks eotaxin-3 expression by oesophageal squamous cells from patients with eosinophilic oesophagitis and GORD. Gut. 2013;62(6):824-32. Epub 20120512. doi: 10.1136/gutjnl-2012-302250. PubMed PMID: 22580413; PMCID: PMC3552049.
- Zhang X, Cheng E, Huo X, Yu C, Zhang Q, Pham TH, Wang DH, Spechler SJ, Souza RF. Omeprazole blocks STAT6 binding to the eotaxin-3 promoter in eosinophilic esophagitis cells. PLoS One. 2012;7(11):e50037. Epub 20121121. doi: 10.1371/journal.pone.0050037. PubMed PMID: 23185525; PMCID: PMC3503709.
- Franciosi JP, Mougey EB, Dellon ES, Gutierrez-Junquera C, Fernandez-Fernandez S, Venkatesh RD, Gupta SK. Proton Pump Inhibitor Therapy for Eosinophilic Esophagitis: History, Mechanisms, Efficacy, and Future Directions. J Asthma Allergy. 2022;15:281-302. Epub 20220226. doi: 10.2147/JAA.S274524. PubMed PMID: 35250281; PMCID: PMC8892718.
- Lucendo AJ, Arias A, Molina-Infante J. Efficacy of Proton Pump Inhibitor Drugs for Inducing Clinical and Histologic Remission in Patients With Symptomatic Esophageal Eosinophilia: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol. 2016;14(1):13-22 e1. Epub 20150803. doi: 10.1016/j.cgh.2015.07.041. PubMed PMID: 26247167.
- Tamarit-Sebastian S, Ferrer-Soler FM, Lucendo AJ. Current options and investigational drugs for the treatment of eosinophilic esophagitis. Expert Opin Investig Drugs. 2022;31(2):193-210. Epub 20220131. doi: 10.1080/13543784.2022.2033207. PubMed PMID: 35072575.
- Gutiérrez-Junquera C, Fernández-Fernández S, Cilleruelo ML, Rayo A, Echeverría L, Quevedo S, Bracamonte T, Román E. High Prevalence of Response to Proton-pump Inhibitor Treatment in Children With Esophageal Eosinophilia. Journal of Pediatric Gastroenterology and Nutrition. 2016;62(5):704-10. doi: https://doi.org/10.1097/MPG.0000000000001019.
- Molina-Infante J, Rodriguez-Sanchez J, Martinek J, van Rhijn BD, Krajciova J, Rivas MD, Barrio J, Moawad FJ, Martinez-Alcala C, Bredenoord AJ, Zamorano J, Dellon ES. Long-Term Loss of Response in Proton Pump Inhibitor-Responsive Esophageal Eosinophilia Is Uncommon and Influenced by CYP2C19 Genotype and Rhinoconjunctivitis. Am J Gastroenterol. 2015;110(11):1567-75. Epub 20150929. doi: 10.1038/ajg.2015.314. PubMed PMID: 26416193.
- Moayyedi P, Eikelboom JW, Bosch J, Connolly SJ, Dyal L, Shestakovska O, Leong D, Anand SS, Stork S, Branch KRH, Bhatt DL, Verhamme PB, O'Donnell M, Maggioni AP, Lonn EM, Piegas LS, Ertl G, Keltai M, Bruns NC, Muehlhofer E, Dagenais GR, Kim JH, Hori M, Steg PG, Hart RG, Diaz R, Alings M, Widimsky P, Avezum A, Probstfield J, Zhu J, Liang Y, Lopez-Jaramillo P, Kakkar AK, Parkhomenko AN, Ryden L, Pogosova N, Dans AL, Lanas F, Commerford PJ, Torp-Pedersen C, Guzik TJ, Vinereanu D, Tonkin AM, Lewis BS, Felix C, Yusoff K, Metsarinne KP, Fox KAA, Yusuf S, Investigators C. Safety of Proton Pump Inhibitors Based on a Large, Multi-Year, Randomized Trial of Patients Receiving Rivaroxaban or Aspirin. Gastroenterology. 2019;157(3):682-91 e2. Epub 20190529. doi: 10.1053/j.gastro.2019.05.056. PubMed PMID: 31152740.
- Nennstiel S, Schlag C. Treatment of eosinophlic esophagitis with swallowed topical corticosteroids. World J Gastroenterol. 2020;26(36):5395-407. doi: 10.3748/wjg.v26.i36.5395. PubMed PMID: 33024392; PMCID: PMC7520613.
- Chen X, Li X. Budesonide Oral Suspension Improves Outcomes in Patients With Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2022;20(5):1188-9. Epub 20210520. doi: 10.1016/j.cgh.2021.05.028. PubMed PMID: 34022453.
- Straumann A, Conus S, Degen L, Felder S, Kummer M, Engel H, Bussmann C, Beglinger C, Schoepfer A, Simon HU. Budesonide is effective in adolescent and adult patients with active eosinophilic esophagitis. Gastroenterology. 2010;139(5):1526-37, 37 e1. Epub 20100801. doi: 10.1053/j.gastro.2010.07.048. PubMed PMID: 20682320.
- Hirano I, Collins MH, Katzka DA, Mukkada VA, Falk GW, Morey R, Desai NK, Lan L, Williams J, Dellon ES, Investigators OS. Budesonide Oral Suspension Improves Outcomes in Patients With Eosinophilic Esophagitis: Results from a Phase 3 Trial. Clin Gastroenterol Hepatol. 2022;20(3):525-34 e10. Epub 20210419. doi: 10.1016/j.cgh.2021.04.022. PubMed PMID: 33887475.
- Dohil R, Newbury R, Fox L, Bastian J, Aceves S. Oral viscous budesonide is effective in children with eosinophilic esophagitis in a randomized, placebo-controlled trial. Gastroenterology. 2010;139(2):418-29. Epub 20100507. doi: 10.1053/j.gastro.2010.05.001. PubMed PMID: 20457157.
- Lucendo AJ, Miehlke S, Schlag C, Vieth M, von Arnim U, Molina-Infante J, Hartmann D, Bredenoord AJ, Ciriza de Los Rios C, Schubert S, Bruckner S, Madisch A, Hayat J, Tack J, Attwood S, Mueller R, Greinwald R, Schoepfer A, Straumann A, International EOSSG. Efficacy of Budesonide Orodispersible Tablets as Induction Therapy for Eosinophilic Esophagitis in a Randomized Placebo-Controlled Trial. Gastroenterology. 2019;157(1):74-86 e15. Epub 20190326. doi: 10.1053/j.gastro.2019.03.025. PubMed PMID: 30922997.
- Willis A, Mani S. Efficacy of Budesonide versus Fluticasone in Children with Eosinophilic Esophagitis. Journal of Allergy and Clinical Immunology. 2022;149(2):AB208. doi: 10.1016/j.jaci.2021.12.683.
- Peterson KA, Thomas KL, Hilden K, Emerson LL, Wills JC, Fang JC. Comparison of esomeprazole to aerosolized, swallowed fluticasone for eosinophilic esophagitis. Dig Dis Sci. 2010;55(5):1313-9. Epub 20090618. doi: 10.1007/s10620-009-0859-4. PubMed PMID: 19533356.
- Schaefer ET, Fitzgerald JF, Molleston JP, Croffie JM, Pfefferkorn MD, Corkins MR, Lim JD, Steiner SJ, Gupta SK. Comparison of oral prednisone and topical fluticasone in the treatment of eosinophilic esophagitis: a randomized trial in children. Clin Gastroenterol Hepatol. 2008;6(2):165-73. doi: 10.1016/j.cgh.2007.11.008. PubMed PMID: 18237866.
- Lee J, Shuker M, Brown-Whitehorn T, Cianferoni A, Gober L, Muir A, Verma R, Liacouras C, Spergel JM. Oral viscous budesonide can be successfully delivered through a variety of vehicles to treat eosinophilic esophagitis in children. J Allergy Clin Immunol Pract. 2016;4(4):767-8. Epub 20160326. doi: 10.1016/j.jaip.2016.02.005. PubMed PMID: 27025298.
- Glowczewski A, Krogulska A. Formulations of Topical Steroids in Eosinophilic Esophagitis-Current Treatment and Emerging Possibilities. J Clin Med. 2022;11(5). Epub 20220307. doi: 10.3390/jcm11051454. PubMed PMID: 35268544; PMCID: PMC8910832.
- Hiremath G, Vaezi M, Gupta S, Acra S, Dellon ES. Management of Uncomplicated Esophageal Food Impaction Varies Substantially between Pediatric and Adult Gastroenterologists Practicing in the US. Gastroenterology. 2017;152(5):S433-S4. doi: 10.1016/S0016-5085(17)31665-7.
- Miehlke S, Schlag C, Storr M, von Arnim U. [Eosinophilic Esophagitis Update: New Guidelines of the European Study Group EUREOS]. Laryngorhinootologie. 2019;98(11):764-75. Epub 20191118. doi: 10.1055/a-0960-6553. PubMed PMID: 31739353.
- Miehlke S, Lucendo AJ, Straumann A, Jan Bredenoord A, Attwood S. Orodispersible budesonide tablets for the treatment of eosinophilic esophagitis: a review of the latest evidence. Ther Adv Gastroenterol. 2020;13:1756284820927282. Epub 20200610. doi: 10.1177/1756284820927282. PubMed PMID: 32565912; PMCID: PMC7288799.
- Fable JM, Fernandez M, Goodine S, Lerer T, Sayej WN. Retrospective Comparison of Fluticasone Propionate and Oral Viscous Budesonide in Children With Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr. 2018;66(1):26-32. doi: 10.1097/MPG.0000000000001626. PubMed PMID: 28489670.
- Albert D, Heifert TA, Min SB, Maydonovitch CL, Baker TP, Chen YJ, Moawad FJ. Comparisons of Fluticasone to Budesonide in the Treatment of Eosinophilic Esophagitis. Dig Dis Sci. 2016;61(7):1996-2001. Epub 20160419. doi: 10.1007/s10620-016-4110-9. PubMed PMID: 27093866.
- Dellon ES, Woosley JT, Arrington A, McGee SJ, Covington J, Moist SE, Gebhart JH, Tylicki AE, Shoyoye SO, Martin CF, Galanko JA, Baron JA, Shaheen NJ. Efficacy of Budesonide vs Fluticasone for Initial Treatment of Eosinophilic Esophagitis in a Randomized Controlled Trial. Gastroenterology. 2019;157(1):65-73 e5. Epub 20190311. doi: 10.1053/j.gastro.2019.03.014. PubMed PMID: 30872104; PMCID: PMC6581596.
- Schroeder S, Fleischer DM, Masterson JC, Gelfand E, Furuta GT, Atkins D. Successful treatment of eosinophilic esophagitis with ciclesonide. J Allergy Clin Immunol. 2012;129(5):1419-21. Epub 20120403. doi: 10.1016/j.jaci.2012.03.007. PubMed PMID: 22480537; PMCID: PMC3816103.
- Nistel M, Nguyen N, Atkins D, Miyazawa H, Burger C, Furuta GT, Menard-Katcher C. Ciclesonide Impacts Clinicopathological Features of Eosinophilic Esophagitis. J Allergy Clin Immunol Pract. 2021;9(11):4069-74. Epub 20210719. doi: 10.1016/j.jaip.2021.06.058. PubMed PMID: 34293498.
- Lee JJ, Fried AJ, Hait E, Yen EH, Perkins JM, Rubinstein E. Topical inhaled ciclesonide for treatment of eosinophilic esophagitis. J Allergy Clin Immunol. 2012;130(4):1011; author reply -2. doi: 10.1016/j.jaci.2012.06.053. PubMed PMID: 23021144; PMCID: PMC3882762.
- Syverson EP, Hait E, McDonald DR, Rubinstein E, Goldsmith JD, Ngo PD, Mitchell PD, Lee JJ. Oral viscous mometasone is an effective treatment for eosinophilic esophagitis. J Allergy Clin Immunol Pract. 2020;8(3):1107-9. Epub 20190912. doi: 10.1016/j.jaip.2019.08.042. PubMed PMID: 31521829.
- Bhardwaj N, Ishmael F, Lehman E, Bethards D, Ruggiero F, Ghaffari G. Effect of topical beclomethasone on inflammatory markers in adults with eosinophilic esophagitis: A pilot study. Allergy Rhinol (Providence). 2017;8(2):85-94. doi: 10.2500/ar.2017.8.0202. PubMed PMID: 28583232; PMCID: PMC5468761.
- Ghaffari G. A randomized double blind placebo controlled crossover study of the effect of swallowed beclomethasone dipropionate on inflammatory markers in adult patients with eosinophilic esophagitis: a pilot study. Annals of Allergy, Asthma & Immunology. 2012;109(5):A19. doi: 10.1016/j.anai.2012.09.018.
- Tomizawa Y, Melek J, Komaki Y, Kavitt RT, Sakuraba A. Efficacy of Pharmacologic Therapy for Eosinophilic Esophagitis: A Systematic Review and Network Meta-Analysis. J Clin Gastroenterol. 2018;52(7):596-606. doi: 10.1097/MCG.0000000000000878. PubMed PMID: 28787360.
- Kumar S, Choi SS, Gupta SK. Eosinophilic esophagitis: current status and future directions. Pediatr Res. 2020;88(3):345-7. Epub 20200121. doi: 10.1038/s41390-020-0770-4. PubMed PMID: 31962343.
- Dellon ES, Spergel JM. Biologics in eosinophilic gastrointestinal diseases. Ann Allergy Asthma Immunol. 2023;130(1):21-7. Epub 20220620. doi: 10.1016/j.anai.2022.06.015. PubMed PMID: 35738437; PMCID: PMC10191215.
- Le Floc'h A, Allinne J, Nagashima K, Scott G, Birchard D, Asrat S, Bai Y, Lim WK, Martin J, Huang T, Potocky TB, Kim JH, Rafique A, Papadopoulos NJ, Stahl N, Yancopoulos GD, Murphy AJ, Sleeman MA, Orengo JM. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Ralpha antibody, is required to broadly inhibit type 2 inflammation. Allergy. 2020;75(5):1188-204. Epub 20200103. doi: 10.1111/all.14151. PubMed PMID: 31838750; PMCID: PMC7317958.
- Dellon ES, Rothenberg ME, Collins MH, Hirano I, Chehade M, Bredenoord AJ, Lucendo AJ, Spergel JM, Aceves S, Sun X, Kosloski MP, Kamal MA, Hamilton JD, Beazley B, McCann E, Patel K, Mannent LP, Laws E, Akinlade B, Amin N, Lim WK, Wipperman MF, Ruddy M, Patel N, Weinreich DR, Yancopoulos GD, Shumel B, Maloney J, Giannelou A, Shabbir A. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N Engl J Med. 2022;387(25):2317-30. doi: 10.1056/NEJMoa2205982. PubMed PMID: 36546624.
- Chehade M, Dellon ES, Spergel JM, Collins MH, Rothenberg ME, Pesek RD, Hirano I, Liu R, Laws E, Mortensen E, Martincova R, Shabbir A, McCann E, Kamal MA, Kosloski MP, Hamilton JD, Samuely C, Lim WK, Wipperman MF, Farrell A, Patel N, Yancopoulos GD, Glotfelty L, Maloney J. Dupilumab for Eosinophilic Esophagitis in Patients 1 to 11 Years of Age. N Engl J Med. 2024;390(24):2239-51. doi: 10.1056/NEJMoa2312282. PubMed PMID: 38924731.
- Straumann A, Conus S, Grzonka P, Kita H, Kephart G, Bussmann C, Beglinger C, Smith DA, Patel J, Byrne M, Simon HU. Anti-interleukin-5 antibody treatment (mepolizumab) in active eosinophilic oesophagitis: a randomised, placebo-controlled, double-blind trial. Gut. 2010;59(1):21-30. doi: 10.1136/gut.2009.178558. PubMed PMID: 19828470.
- Dellon ES, Peterson KA, Mitlyng BL, Iuga A, Bookhout CE, Cortright LM, Walker KB, Gee TS, McGee SJ, Cameron BA, Galanko JA, Woosley JT, Eluri S, Moist SE, Hirano I. Mepolizumab for treatment of adolescents and adults with eosinophilic oesophagitis: a multicentre, randomised, double-blind, placebo-controlled clinical trial. Gut. 2023;72(10):1828-37. Epub 20230709. doi: 10.1136/gutjnl-2023-330337. PubMed PMID: 37423717; PMCID: PMC11315207.
- Spergel JM, Rothenberg ME, Collins MH, Furuta GT, Markowitz JE, Fuchs G, 3rd, O'Gorman MA, Abonia JP, Young J, Henkel T, Wilkins HJ, Liacouras CA. Reslizumab in children and adolescents with eosinophilic esophagitis: results of a double-blind, randomized, placebo-controlled trial. J Allergy Clin Immunol. 2012;129(2):456-63, 63 e1-3. Epub 20111228. doi: 10.1016/j.jaci.2011.11.044. PubMed PMID: 22206777.
- Walsh GM. Reslizumab, a humanized anti-IL-5 mAb for the treatment of eosinophil-mediated inflammatory conditions. Curr Opin Mol Ther. 2009;11(3):329-36. PubMed PMID: 19479666.
- Stein ML, Villanueva JM, Buckmeier BK, Yamada Y, Filipovich AH, Assa'ad AH, Rothenberg ME. Anti-IL-5 (mepolizumab) therapy reduces eosinophil activation ex vivo and increases IL-5 and IL-5 receptor levels. J Allergy Clin Immunol. 2008;121(6):1473-83, 83 e1-4. Epub 20080414. doi: 10.1016/j.jaci.2008.02.033. PubMed PMID: 18410960; PMCID: PMC2749495.
- Otani IM, Anilkumar AA, Newbury RO, Bhagat M, Beppu LY, Dohil R, Broide DH, Aceves SS. Anti-IL-5 therapy reduces mast cell and IL-9 cell numbers in pediatric patients with eosinophilic esophagitis. J Allergy Clin Immunol. 2013;131(6):1576-82. Epub 20130425. doi: 10.1016/j.jaci.2013.02.042. PubMed PMID: 23623266; PMCID: PMC3699422.
- Stein ML, Collins MH, Villanueva JM, Kushner JP, Putnam PE, Buckmeier BK, Filipovich AH, Assa'ad AH, Rothenberg ME. Anti-IL-5 (mepolizumab) therapy for eosinophilic esophagitis. J Allergy Clin Immunol. 2006;118(6):1312-9. Epub 20061107. doi: 10.1016/j.jaci.2006.09.007. PubMed PMID: 17157662.
- Rothenberg ME, Dellon ES, Collins MH, Bredenoord AJ, Hirano I, Peterson KA, Brooks L, Caldwell JM, Fjallbrant H, Grindebacke H, Ho CN, Keith M, McCrae C, Sinibaldi D, White WI, Datto CJ, Investigators MT. Eosinophil Depletion with Benralizumab for Eosinophilic Esophagitis. N Engl J Med. 2024;390(24):2252-63. doi: 10.1056/NEJMoa2313318. PubMed PMID: 38924732.
- Ketchem CJ, Starling AS. Insights into the natural history and disease course of eosinophilic esophagitis. Ann Allergy Asthma Immunol. 2025;135(2):155-61. Epub 20250329. doi: 10.1016/j.anai.2025.03.019. PubMed PMID: 40164282.
- Loizou D, Enav B, Komlodi-Pasztor E, Hider P, Kim-Chang J, Noonan L, Taber T, Kaushal S, Limgala R, Brown M, Gupta R, Balba N, Goker-Alpan O, Khojah A, Alpan O. A pilot study of omalizumab in eosinophilic esophagitis. PLoS One. 2015;10(3):e0113483. Epub 20150319. doi: 10.1371/journal.pone.0113483. PubMed PMID: 25789989; PMCID: PMC4366078.
- Clayton F, Fang JC, Gleich GJ, Lucendo AJ, Olalla JM, Vinson LA, Lowichik A, Chen X, Emerson L, Cox K, O'Gorman MA, Peterson KA. Eosinophilic esophagitis in adults is associated with IgG4 and not mediated by IgE. Gastroenterology. 2014;147(3):602-9. Epub 20140604. doi: 10.1053/j.gastro.2014.05.036. PubMed PMID: 24907494.
- Rothenberg ME, Wen T, Greenberg A, Alpan O, Enav B, Hirano I, Nadeau K, Kaiser S, Peters T, Perez A, Jones I, Arm JP, Strieter RM, Sabo R, Gunawardena KA. Intravenous anti-IL-13 mAb QAX576 for the treatment of eosinophilic esophagitis. J Allergy Clin Immunol. 2015;135(2):500-7. Epub 20140913. doi: 10.1016/j.jaci.2014.07.049. PubMed PMID: 25226850.
- Hirano I, Collins MH, Assouline-Dayan Y, Evans L, Gupta S, Schoepfer AM, Straumann A, Safroneeva E, Grimm M, Smith H, Tompkins CA, Woo A, Peach R, Frohna P, Gujrathi S, Penenberg DN, Li C, Opiteck GJ, Olson A, Aranda R, Rothenberg ME, Dellon ES, Group HS. RPC4046, a Monoclonal Antibody Against IL13, Reduces Histologic and Endoscopic Activity in Patients With Eosinophilic Esophagitis. Gastroenterology. 2019;156(3):592-603 e10. Epub 20181102. doi: 10.1053/j.gastro.2018.10.051. PubMed PMID: 30395812.
- Dellon ES, Charriez CM, Zhang S, Falk GW, Oliva S, Ma C, Siffledeen J, Schroeder S, Philpott H, Vanuytsel T, Abe Y, Li K, Zema CL, Venkatasamy A, Yeshokumar AK, Oh YS, Schoepfer A. Cendakimab in Adults and Adolescents with Eosinophilic Esophagitis. NEJM Evid. 2025;4(10):EVIDoa2500095. Epub 20250923. doi: 10.1056/EVIDoa2500095. PubMed PMID: 40985784.
- Kiwamoto T, Kawasaki N, Paulson JC, Bochner BS. Siglec-8 as a drugable target to treat eosinophil and mast cell-associated conditions. Pharmacol Ther. 2012;135(3):327-36. Epub 20120627. doi: 10.1016/j.pharmthera.2012.06.005. PubMed PMID: 22749793; PMCID: PMC3587973.
- Hirano I, Peterson K, Murray J, Dellon E, Falk G, Gonsalves N, Chehade M, Leung J, Genta R, Khoury P, Bledsoe A, Shaw C, Rasmussen H, Singh B, Chang A, Kamboj A, Rothenberg M. AK002, an Anti-Siglec-8 Antibody, Depletes Tissue Eosinophils and Improves Dysphagia Symptoms in Patients with Eosinophilic Esophagitis. Journal of Allergy and Clinical Immunology. 2020;145(2):AB167. doi: 10.1016/j.jaci.2019.12.343.
- Dellon E, Chehade M, Genta RM, Leiman DA, Peterson KA, Spergel J, Wechsler J, Bortey E, Chang AT, Hirano I. S446 Results from KRYPTOS, a Phase 2/3 Study of Lirentelimab (AK002) in Adults and Adolescents With EoE. Official journal of the American College of Gastroenterology | ACG. 2022;117(10S).
- Straumann A, Bussmann C, Conus S, Beglinger C, Simon HU. Anti-TNF-alpha (infliximab) therapy for severe adult eosinophilic esophagitis. J Allergy Clin Immunol. 2008;122(2):425-7. doi: 10.1016/j.jaci.2008.06.012. PubMed PMID: 18678345.
- McLean LP, Cross RK. Integrin antagonists as potential therapeutic options for the treatment of Crohn's disease. Expert Opin Investig Drugs. 2016;25(3):263-73. doi: 10.1517/13543784.2016.1148137. PubMed PMID: 26822204; PMCID: PMC4926164.
- Taft TH, Mutlu EA. The Potential Role of Vedolizumab in Concomitant Eosinophilic Esophagitis and Crohn's Disease. Clin Gastroenterol Hepatol. 2018;16(11):1840-1. doi: 10.1016/j.cgh.2018.06.022. PubMed PMID: 30343868.
- Nhu QM, Chiao H, Moawad FJ, Bao F, Konijeti GG. The Anti-alpha4beta7 Integrin Therapeutic Antibody for Inflammatory Bowel Disease, Vedolizumab, Ameliorates Eosinophilic Esophagitis: a Novel Clinical Observation. Am J Gastroenterol. 2018;113(8):1261-3. Epub 20180612. doi: 10.1038/s41395-018-0145-1. PubMed PMID: 29895980.
- Dellon ES, Collins MH, Bredenoord AJ, Philpott H, Biedermann L, Dulcine M, Nguyen-Cleary T, Su C, Yu J, Tan H, Cataldi F, Wu J, Wang W, Clax P, Woolcott JC, Hirano I. Etrasimod as a treatment for eosinophilic oesophagitis (VOYAGE): a double-blind, placebo-controlled, randomised, phase 2 trial. Lancet Gastroenterol Hepatol. 2025;10(7):622-33. Epub 20250514. doi: 10.1016/S2468-1253(25)00062-7. PubMed PMID: 40381637.
- Oliva S, Aceves SS, Zevit N, Rothenberg ME, Furuta GT, Dellon ES. Crafting a Therapeutic Pyramid for Eosinophilic Esophagitis in the Age of Biologics. Clin Gastroenterol Hepatol. 2024;22(9):1763-9. Epub 20240511. doi: 10.1016/j.cgh.2024.04.020. PubMed PMID: 38735510.
- Schoepfer AM, Safroneeva E. Pharmacologic Treatment of Eosinophilic Esophagitis: Efficacious, Likely Efficacious, and Failed Drugs. Inflamm Intest Dis. 2024;9(1):199-209. Epub 20240726. doi: 10.1159/000540275. PubMed PMID: 39474328; PMCID: PMC11521425.
- Aceves SS, Alexander JA, Baron TH, Bredenoord AJ, Day L, Dellon ES, Falk GW, Furuta GT, Gonsalves N, Hirano I, Konda VJA, Lucendo AJ, Moawad F, Peterson KA, Putnam PE, Richter J, Schoepfer AM, Straumann A, McBride DL, Sharma P, Katzka DA. Endoscopic approach to eosinophilic esophagitis: American Society for Gastrointestinal Endoscopy Consensus Conference. Gastrointest Endosc. 2022;96(4):576-92 e1. Epub 20220811. doi: 10.1016/j.gie.2022.05.013. PubMed PMID: 35965102.
- Greenberg SB, Ocampo AA, Xue Z, Chang NC, Thakkar KP, Reddy SB, Lee CJ, Ketchem CJ, Redd WD, Eluri S, Reed CC, Dellon ES. Increasing Rates of Esophageal Stricture and Dilation Over 2 Decades in Eosinophilic Esophagitis. Gastro Hep Adv. 2023;2(4):521-3. Epub 20221230. doi: 10.1016/j.gastha.2022.12.006. PubMed PMID: 37293573; PMCID: PMC10249492.
- Moawad FJ, Molina-Infante J, Lucendo AJ, Cantrell SE, Tmanova L, Douglas KM. Systematic review with meta-analysis: endoscopic dilation is highly effective and safe in children and adults with eosinophilic oesophagitis. Aliment Pharmacol Ther. 2017;46(2):96-105. Epub 20170517. doi: 10.1111/apt.14123. PubMed PMID: 28513085.
- Dougherty M, Runge TM, Eluri S, Dellon ES. Esophageal dilation with either bougie or balloon technique as a treatment for eosinophilic esophagitis: a systematic review and meta-analysis. Gastrointest Endosc. 2017;86(4):581-91 e3. Epub 20170428. doi: 10.1016/j.gie.2017.04.028. PubMed PMID: 28461094; PMCID: PMC5601027.
- Josino IR, Madruga-Neto AC, Ribeiro IB, Guedes HG, Brunaldi VO, de Moura DTH, Bernardo WM, de Moura EGH. Endoscopic Dilation with Bougies versus Balloon Dilation in Esophageal Benign Strictures: Systematic Review and Meta-Analysis. Gastroenterol Res Pract. 2018;2018:5874870. Epub 20180715. doi: 10.1155/2018/5874870. PubMed PMID: 30116265; PMCID: PMC6079446.
- Menard-Katcher C, Furuta GT, Kramer RE. Dilation of Pediatric Eosinophilic Esophagitis: Adverse Events and Short-term Outcomes. J Pediatr Gastroenterol Nutr. 2017;64(5):701-6. doi: 10.1097/MPG.0000000000001336. PubMed PMID: 28055990; PMCID: PMC6136143.
- Hiremath GS, Hameed F, Pacheco A, Olive A, Davis CM, Shulman RJ. Esophageal Food Impaction and Eosinophilic Esophagitis: A Retrospective Study, Systematic Review, and Meta-Analysis. Dig Dis Sci. 2015;60(11):3181-93. Epub 20150612. doi: 10.1007/s10620-015-3723-8. PubMed PMID: 26065368; PMCID: PMC4624046.
- Pasha SF, DiBaise JK, Kim HJ, De Petris G, Crowell MD, Fleischer DE, Sharma VK. Patient characteristics, clinical, endoscopic, and histologic findings in adult eosinophilic esophagitis: a case series and systematic review of the medical literature. Dis Esophagus. 2007;20(4):311-9. doi: 10.1111/j.1442-2050.2007.00721.x. PubMed PMID: 17617880.
- Singh B, Nijhawan S, Shwetanshu Narayan K, Kumar A. Endoscopic management of ingested foreign bodies and food impaction in esophagus. Journal of Digestive Endoscopy. 2015;6(3):96-100.
- Birk M, Bauerfeind P, Deprez PH, Hafner M, Hartmann D, Hassan C, Hucl T, Lesur G, Aabakken L, Meining A. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016;48(5):489-96. Epub 20160210. doi: 10.1055/s-0042-100456. PubMed PMID: 26862844.
- Kramer RE, Lerner DG, Lin T, Manfredi M, Shah M, Stephen TC, Gibbons TE, Pall H, Sahn B, McOmber M, Zacur G, Friedlander J, Quiros AJ, Fishman DS, Mamula P, North American Society for Pediatric Gastroenterology H, Nutrition Endoscopy C. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr. 2015;60(4):562-74. doi: 10.1097/MPG.0000000000000729. PubMed PMID: 25611037.
- Lightdale JR, Liu QY, Sahn B, Troendle DM, Thomson M, Fishman DS, Endoscopy N, Procedures C. Pediatric Endoscopy and High-risk Patients: A Clinical Report From the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr. 2019;68(4):595-606. doi: 10.1097/MPG.0000000000002277. PubMed PMID: 30664560; PMCID: PMC8597353.
- Barlowe TS, Redd WD, Xue AZ, Kiran A, McCallen JD, Eluri S, Reed CC, Dellon ES. Performing Esophageal Biopsies Is Safe During Upper Endoscopy for Food Impaction but Are Underperformed in Certain Populations. Dig Dis Sci. 2024;69(10):3844-52. Epub 20240813. doi: 10.1007/s10620-024-08590-8. PubMed PMID: 39136838.
- Runge TM, Eluri S, Cotton CC, Burk CM, Woosley JT, Shaheen NJ, Dellon ES. Causes and Outcomes of Esophageal Perforation in Eosinophilic Esophagitis. J Clin Gastroenterol. 2017;51(9):805-13. doi: 10.1097/MCG.0000000000000718. PubMed PMID: 27680593; PMCID: PMC5368035.
- Arias-Gonzalez L, Rey-Iborra E, Ruiz-Ponce M, Laserna-Mendieta EJ, Arias A, Lucendo AJ. Esophageal perforation in eosinophilic esophagitis: A systematic review on clinical presentation, management and outcomes. Dig Liver Dis. 2020;52(3):245-52. Epub 20191210. doi: 10.1016/j.dld.2019.10.019. PubMed PMID: 31836305.
- Xu X, Chen H, Chen Y, Fan L. Application of artificial intelligence in eosinophilic esophagitis. Front Immunol. 2025;16:1712113. Epub 20251110. doi: 10.3389/fimmu.2025.1712113. PubMed PMID: 41293175; PMCID: PMC12640925.
- Castagnaro E, Felici E, Spaccapelo R, Amoroso M, Moretti D, Saab JP, Stassaldi A, Tassone A, Borrelli O, De Bortoli N, Corso GD, Gaynor E, Goh L, Oliva S, Rea F, Renzo S, Romano C, Savarino EV, Visaggi P. Systematic Review: Use of Artificial Intelligence and Unmet Needs in Eosinophilic Oesophagitis. Aliment Pharmacol Ther. 2025;62(2):110-27. Epub 20250605. doi: 10.1111/apt.70222. PubMed PMID: 40474554.
- Ketchem CJ, Gabryszewski SJ, Rothenberg ME. Artificial intelligence in the detection and management of eosinophilic gastrointestinal diseases: Applications, challenges, and future outlook. J Allergy Clin Immunol. 2026;157(1):56-8. Epub 20250904. doi: 10.1016/j.jaci.2025.08.020. PubMed PMID: 40914297; PMCID: PMC12543360.
- Shoda T, Wen T, Aceves SS, Abonia JP, Atkins D, Bonis PA, Caldwell JM, Capocelli KE, Carpenter CL, Collins MH, Dellon ES, Eby MD, Gonsalves N, Gupta SK, Falk GW, Hirano I, Menard-Katcher P, Kuhl JT, Krischer JP, Leung J, Mukkada VA, Spergel JM, Trimarchi MP, Yang GY, Zimmermann N, Furuta GT, Rothenberg ME, Consortium of Eosinophilic Gastrointestinal Disease R. Eosinophilic oesophagitis endotype classification by molecular, clinical, and histopathological analyses: a cross-sectional study. Lancet Gastroenterol Hepatol. 2018;3(7):477-88. Epub 20180503. doi: 10.1016/S2468-1253(18)30096-7. PubMed PMID: 29730081; PMCID: PMC5997568.
- Mougey EB, Williams A, Coyne AJK, Gutierrez-Junquera C, Fernandez-Fernandez S, Cilleruelo ML, Rayo A, Echeverria L, Roman E, Gonzalez Lois C, Chao M, Al-Atrash H, Lima JJ, Franciosi JP. CYP2C19 and STAT6 Variants Influence the Outcome of Proton Pump Inhibitor Therapy in Pediatric Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr. 2019;69(5):581-7. doi: 10.1097/MPG.0000000000002480. PubMed PMID: 31490856; PMCID: PMC6855320.
- Scodellaro S, Bortolin KA, Marcon MA, Verstegen RHJ, Da Silva S, Ito S, Lewis T, Jones NL, Cohn I, Hulst JM. Optimizing proton-pump inhibitor therapy in paediatric eosinophilic esophagitis through CYP2C19 pharmacogenetic testing. J Can Assoc Gastroenterol. 2025;8(3):89-96. Epub 20250313. doi: 10.1093/jcag/gwaf003. PubMed PMID: 40567296; PMCID: PMC12188439.
- Canas JA, Tabares A, Barbero C, Garcia-Sanchez D, Sastre B, Rodrigo-Munoz JM, Mahillo-Fernandez I, Rayo A, Borrell B, Cilleruelo ML, Roman E, Fernandez-Fernandez S, Gutierrez-Junquera C, Del Pozo V. Proton-pump Inhibitor Response Prediction Using Esophageal microRNAs in Children With Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr. 2020;71(6):755-63. doi: 10.1097/MPG.0000000000002957. PubMed PMID: 33003164; PMCID: PMC7752232.
- Dellon ES, Guo R, McGee SJ, Hamilton DK, Nicolai E, Covington J, Moist SE, Arrington A, Wright BL, Burks AW, Vickery BP, Kulis M. A Novel Allergen-Specific Immune Signature-Directed Approach to Dietary Elimination in Eosinophilic Esophagitis. Clin Transl Gastroenterol. 2019;10(12):e00099. doi: 10.14309/ctg.0000000000000099. PubMed PMID: 31789931; PMCID: PMC6970559.