
Frequently Asked Questions
Eosinophilic Gastrointestinal Disease (EGID) Diagnosis
Does diagnosis and/or treatment of EGID require a specialist?
A proper diagnosis of EGID is made by a gastroenterologist and pathologist. Once diagnosed, it is important to discuss a treatment plan, including medications and/or dietary therapies, as well as the frequency of follow-up care/evaluation. Often, your gastroenterologist will collaborate with other specialists, including the following:
- Allergist/Immunologist – Allergy testing is often used to help identify food/environmental allergies and guide diet management.
- Registered Dietitian – Because a diagnosis of EGID usually requires prolonged restriction/elimination of foods from diets, it is recommended that patients/caregivers consult with a dietitian to ensure appropriate calories, vitamins, and nutrients are maintained and that the elimination diet is being performed correctly.
- Clinical Psychologist – Following diagnosis, it can be helpful for some patients to consult with a psychologist to discuss coping strategies as they adapt to living with/managing a chronic disease.
- Feeding Therapist – Following diagnosis, it can be helpful for some patients to consult with a feeding therapist to discuss coping strategies as they learn or re-learn ways to eat solid foods.
How can we better identify EGIDs early, so we are not waiting for symptoms to arise before we know there is a problem?
- Currently, there are no widely accepted screening tests for EGIDs.
- EoE is a chronic disease that progresses from inflammation to scarring over time.
- The ideal screening test for an EGID should:
- Be inexpensive and easy to administer.
- Cause minimal discomfort or harm to the patient.
- Give valid results.
- Detect the disease early.
- Several screening tests for EoE are in development including the esophageal string test, transnasal endoscopy, Cytosponge, nuclear medicine studies, and blood tests.
- The medical history, family history, and clinical symptoms may help identify patients at higher risk for EoE and scarring.
Are there any other methods to diagnose/monitor EGID other than any endoscopy?
Currently, endoscopy with biopsies is the only reliable method to diagnose and evaluate EGID. Research is underway to develop less invasive methods.
Eosinophilic Gastrointestinal Disease (EGID) Management and Treatment
Does diagnosis and/or treatment of EGID require a specialist?
A proper diagnosis of EGID is made by a gastroenterologist and pathologist. Once diagnosed, it is important to discuss a treatment plan, including medications and/or dietary therapies, as well as the frequency of follow-up care/evaluation. Often, your gastroenterologist will collaborate with other specialists, including the following:
- Allergist/Immunologist – An allergist will evaluate for coexisting allergic conditions such as IgE-mediated food allergy, eczema, asthma, and allergic rhinitis. Evaluation may include allergy testing. Depending on the history and the coexisting allergic conditions, the allergist will weigh in about appropriate treatment strategies.
- Registered Dietitian – Because a diagnosis of EGID usually requires prolonged restriction/elimination of foods from diets, it is recommended that patients/caregivers consult with a dietitian to ensure appropriate calories, vitamins, and nutrients are maintained and that the elimination diet is being performed correctly.
- Clinical Psychologist – Following diagnosis, it can be helpful for some patients to consult with a psychologist to discuss coping strategies as they adapt to living with/managing a chronic disease.
- Feeding Therapist – Following diagnosis, it can be helpful for some patients to consult with a feeding therapist to discuss coping strategies as they learn or re-learn ways to eat solid foods.
Are treatment plans for all EGIDs the same?
Treatment approaches differ across EGIDs. While evidence-based consensus guidelines exist for the diagnosis and management of EoE, treatment guidance for non-EoE EGIDs are evolving. For EoE, therapies include dietary management, proton pump inhibitor therapy, swallowed topical corticosteroids, and the biologic agent dupilumab. For non-EoE EGIDs, dietary therapy and systemic or locally acting corticosteroids are used, with treatment individualized based on disease location, severity, and patient response.
What is dietary management?
Because EGIDs are often triggered by certain foods, your healthcare provider may prescribe dietary management. This may include elimination diets in which all foods that tested positive on allergy tests are avoided, common allergy-causing food elimination in which likely causative foods are avoided, elemental diet in which a patient drinks only an amino acid formula (or has it delivered via a feeding tube), and food trial in which specific foods are removed from the diet and then added back one at a time to determine the reaction.
How effective is allergy testing in identifying food triggers for EGID?
Although allergy tests can be useful in helping guide diet therapies, these tests may produce either false-positive or false-negative results, and when used alone, are not sufficient to identify specific food triggers that may be causing the increased eosinophil activity driving the disease. Food triggers can usually only be identified following a methodical food trial process, involving the elimination and/or reintroduction of foods, followed by endoscopy/biopsies to confirm disease remission/activity.
Can biologics used for the treatment of inflammatory bowel disease be used to treat EGIDs
- There are several different biologic medications used for the treatment of inflammatory bowel disease. Some of these include the following:
- Anti-TNFα agents [eg, infliximab (Remicade), adalimumab (Humira)]
- Anti-α4β7 integrin agents [eg, vedolizumab (Entyvio)]
- JAK1/3 inhibitors [eg, tofacitinib (Xeljanz)]
- Data supporting the use of anti-TNFα agents, anti-α4β7 integrin agents, and JAK 1/3 inhibitors for EGIDs is limited.
- A handful of small case series and case reports suggest these medications may be helpful depending on the individual and the parts of the gastrointestinal tract affected. Others have not been as supportive.
- None of these medications are approved by the FDA for the treatment of EGIDs. Additional studies are needed to evaluate the safety and efficacy of these medications.
Is there any consensus as to how frequently a child with EGID should undergo an endoscopic procedure? What about an adult?
The frequency of endoscopic evaluation is part of the individualized treatment plan that you will want to discuss with your gastroenterologist/EGID care team. In some cases, children/adults going through food trials to help identify food triggers have endoscopies performed at varying intervals. A similar interval is common if/when a new medicine is introduced in order to assess its efficacy. Asymptomatic patients, those whose disease is believed to be managed or in remission, may be evaluated when deemed appropriate by their doctor.
Why are there no formula alternatives for patients with EGIDs who are also sensitive to sugar?
- EGIDs are triggered by food proteins and can be treated with hypoallergenic elemental formulas that only contain amino acids—the building blocks of proteins.
- Corn syrup solids are the main source of carbohydrates (i.e., sugars) in elemental formulas.
- The refining and conversion process of corn increases absorption and removes protein from the syrup solids. In this form, corn generally does not cause allergic reactions.
- Amino acids increase the osmolality (concentration) of elemental formula. Increased osmolality can cause symptoms of diarrhea and bloating. By adding corn syrup solids, manufacturers maximize calories without significantly increasing osmolality.
- Some patients may have intolerances to carbohydrates in elemental formulas due to enzyme deficiencies (e.g., maltase deficiency).
- The high carbohydrate content of these formulas may increase blood sugar levels, but more research is needed to understand long-term effects.
Why aren’t functional medicine approaches used for the treatment of EGIDs?
- Functional medicine is a type of alternative medicine that focuses on identifying and addressing the root cause of a disease.
- The use of functional or complementary medicine products is common amongst patients and families and should be discussed during clinic visits.
- Traditional Chinese medicine may help for treating other allergic diseases, while the data on acupuncture is more limited.
- There are no published, quality studies evaluating functional or alternative medicine as treatments for EGIDs.
For patients with non-esophageal EGIDs and limited healthcare resources, what are the most important things they should or should not do?
- There are multiple barriers to care for EGIDs because symptoms are non-specific, misdiagnosis is common, and care requires access to specialists.
- To overcome these obstacles, it is important to establish a medical team for your EGID treatment.
- Use telemedicine where available.
- Create a self-management plan with your specialist(s).
- Coordinate your self-management plan with your local primary care provider.
- Self-management plans for EGIDs will depend on your treatment approach.
- Diet - Find a dietician (where possible) and avoid specific IgE or skin testing to guide EGID diet elimination. Consider the costs and lifestyle changes associated with diet elimination.
- Steroids – be consistent with dosing as prescribed and notify your providers about any side effects. Typically, topical steroids are used for maintenance treatment and high-dose oral systemic steroids are only used as a rescue treatment for flares due to possible side effects.
- If you have other conditions, make sure they are treated and prioritize stress management to improve your EGID and your quality of life.&
- Join patient advocacy groups (APFED, ausEE, CURED, EFC, EOS Network) and access online resources through their websites.
Eosinophilic Gastrointestinal Disease (EGID) Development
What are some of the risk factors that contribute to developing EGID?
- Studies of identical vs. fraternal twins with EoE suggest that environmental factors are important for the development of EoE.
- Early life exposures may influence the microbes that colonize the infant gut.
- Antibiotic and antacid exposure are risk factors for EoE.
- For antibiotics:
- We see a higher risk of EoE if a mother takes antibiotics during the third trimester.
- After birth, the risk for EoE increases the earlier and the more antibiotics are prescribed in infancy.
- For acid suppressants:
- We see increased risk for EoE if either a pregnant mother or infant has been prescribed antacids.
- Future studies are needed to understand the mechanisms whereby these risk factors contribute to EoE development.
I have one child with an EGID. What is the risk that my other children may have/develop an EGID?
The presence of an EGID in the child increases the risk in another child, but the risk still remains low. For EoE, there is about a 2.4% risk of EoE in siblings of an EoE patient.
Will EGID (EoC, EoE, and EoG) ever go away? Will it get worse?
EGID is a chronic disease that usually requires long-term follow-up and treatment. It is common for patients to experience periods when the disease flares up and causes symptoms, followed by periods of remission when there are no symptoms experienced.
Can you grow out of EoE or other EGIDs?
- Most patients require ongoing, life-long treatment for EoE to control inflammation and prevent scarring.
- The absence of symptoms does not necessarily mean that inflammation is controlled.
- EoE may be outgrown in a small subset of patients (< 5%).
- Eosinophilic inflammation affecting the stomach or intestines may be more likely to resolve.
- The factors that may lead to long-term remission in EGIDs are unknown.
- CEGIR is investigating the natural history of EGIDs through an ongoing cohort study.
Can an allergy cause EGID?
The cause of EGID is not fully understood, but it is often seen in people that have allergic conditions or a family history of atopy. An immune response to food is typically involved in causing EGID.
Can an injury cause EGID?
No. EGID is not caused by an injury.
Have changes in farming practices or food manufacturing, processing, and packaging increased the number of EGIDs?
- The incidence and prevalence of EoE has increased in the last 30 years.
- Several changes have been introduced in farming practices and food production since the 1950’s:
- Mechanization, fertilizers, pesticides (eg, glyphosates), and genetically modified seeds have been used more.
- Antibiotic use has increased and there are more animals in feedlots.
- Preservatives and plastics (eg, phthalates) have been introduced to preserve and package foods.
- It is unknown whether any of these changes have contributed to the increase in EGIDs.
- Environmental exposure to some pesticides may be associated with increases in food allergy, but additional research is needed to identify causal relationships between chemical and antibiotic exposures in the food supply and EGIDs.
Are there ways to prevent EGIDs if they run in the family?
- Several risk factors have been associated with EGIDs including the use of acid suppressing agents (eg, proton pump inhibitors, H2 blockers), early antibiotic exposure, delivery by C-section, prematurity, admission to the NICU, maternal fever, and infant formula use.
- A study in mice suggests detergents may contribute to EoE development.
- Having a cat or dog may be associated with a decreased risk for EoE.
- Each of these factors may have effects on the microbiome.
- We don’t know whether any of these factors cause or prevent EGIDs.
- Possible ways to prevent EGIDs may include:
- Focusing on a mother’s health and her pregnancy care.
- Breastfeeding through the first 6 months of life.
- Appropriate use of acid suppressing medications and antibiotics.
- Getting enough vitamin D, particularly in cold regions with less sunlight.
- Encouraging a well-balanced diet and healthy lifestyle.
- More research is needed to identify the causes of EGIDs and ways to prevent them.
Is it harmful to use laxatives long term if you have EGIDs?
- Constipation has been reported in EGIDs but is not a common feature.
- There are two main types of laxatives used for constipation:
- Stool softeners
- Stimulant laxatives
- There are conflicting results and very few studies regarding long-term safety of stimulant laxatives, so additional research is needed.
- Possible side effects of laxatives include abdominal pain, gassiness, and loose stools.
- Before using fiber as a laxative, speak to your doctor if you have a history of narrowing or stricture in the gastrointestinal tract.
What advances are in the pipeline for diagnosing and monitoring EGIDs?
- Efforts are underway to develop consensus criteria for diagnosis of EGIDs affecting the stomach and intestines.
- Eosinophils and their granule proteins have been used to assess inflammation and disease activity in EGIDs.
- T cells and mast cells are also being evaluated as markers for EGIDs.
- Food-specific IgG4 and IgG4-producing cells have been shown to be elevated in EGIDs.
- Gene expression panels analyzing markers in gastrointestinal biopsies and the blood may distinguish patients with EGIDs.
- Imaging (eg, CT, MRI) or endoscopy findings may be useful in addition to gastrointestinal biopsies.
- Additional research is needed to identify which markers are best for diagnosis or long.
- Ongoing research will continue to refine diagnostic and monitoring criteria, in particular for non-EoE EGIDs in adults.
- Research studies are evaluating whether blood immune cells respond to specific food proteins when tested outside the body.
What is the role of the microbiome in EGIDs?
- The microbiome consists of the trillions of bacteria, fungi, viruses, and other microorganisms that live on and within us.
- An imbalance in the microbiome, called dysbiosis, is associated with allergic diseases such as asthma and eczema
- Early-life exposures affecting the microbiome (eg, antibiotic use, Cesarean delivery, preterm delivery) are associated with EoE.
- Previous studies of the microbiome in EGIDs have primarily focused on the bacteria present in EoE.
- The healthy esophagus has a unique microbiome with increased numbers of gram-positive bacteria from the phylum Firmicutes.
- Studies in mice show the esophageal microbiome is dictated by the unique esophageal microenvironment.
- EoE may be associated with increased numbers of bacteria in the esophagus.
- Gram-negative bacteria (eg, Prevotella, Neisseria, Haemophilus species) may be increased in the esophagus of patients with EoE.
- The stool microbiome is not a good non-invasive test for EoE because, so far, researchers have not observed any differences in the stool microbiome of patients with EoE compared to patients without EoE.
- Additional studies are needed to determine if changing the microbiome (eg, probiotics) can be used to prevent or treat EGIDs.
How do duodenal ulcers and hemoglobin levels play a role in eosinophilic gastritis or duodenitis?
- Ulcers are surface injuries in the lining of the GI tract.
- Ulcers are rare but can cause dangerous complications in patients with eosinophilic gastritis or duodenitis, like upper GI bleeding or gastrointestinal perforation.
- Anemia is a low red blood cell count leading to symptoms like fatigue, palpitations, or dizziness.
- Anemia is more common than ulcers, and can develop slowly over time or quickly in the setting of bleeding.
- Ulcers or anemia typically develop in the setting of active tissue eosinophilic inflammation and can occur at diagnosis or later.
- Management includes treating the ulcer or anemia, but also treating the eosinophilic inflammation.
Eosinophilic Gastrointestinal Disease (EGID) Research
What research is being done to prevent EGIDs?
- There are four stages of disease prevention:
- Reducing risk factors for all patients.
- Preventing EGIDs in healthy, but susceptible patients.
- Identifying patients who have early signs of EGIDs without symptoms.
- Reducing disease severity in patients diagnosed with EGIDs.
- The increase in EGIDs is likely due to a combination of factors including specific exposures, patient characteristics, and the environment.
- Potential early life exposures may include prematurity, cesarean section delivery, lack of breastfeeding, and acid blocker or antibiotic use in infancy.
- Patient factors include other allergic diseases, poor esophageal barrier function, and increased susceptibility to inflammation and scarring.
- Potential environmental factors include cold, arid climates.
- Future studies are needed to identify cause and effect relationships between these factors and the development of EGIDs.
Are access to healthcare and socioeconomic factors being studied in EGIDs?
- Existing data is limited, but some tools are available to evaluate how socioeconomic factors and access to healthcare affect EGID care.
- The Childhood Opportunity Index (COI) measures and maps the quality of resources and conditions that matter for children to develop in a healthy way in the neighborhoods where they live.
- The COI has been used to study pediatric asthma.
- Factors including high foreclosure rates and low levels of education may increase the risk for asthma-related hospitalization and need for healthcare.
- Living closer to a healthcare facility may decrease the risk for asthma-related hospitalization and need for healthcare.
- The COI may be a tool that can help us understand how access to healthcare, education, and socioeconomic status affect patients with EGIDs in the US.
- CEGIR is actively researching how these factors influence care of patients with EoE who go to the emergency room for a food impaction.
Eosinophilic Gastrointestinal Disease (EGID) Symptoms and Other Conditions
Do all patients experience similar symptoms?
EGIDs are individualized diseases, and there are variances in triggers that cause flares and symptoms that patients exhibit. Symptoms may vary depending on which subset of an EGID you have, and your age. For example, with EoE, it is more common for children to experience vomiting while adults are more likely to present with difficulty swallowing.
Will EGID impact a child's growth and development?
Prior to diagnosis, many children with EGID experience delays in growth and development due to poor diets/nutritional deficiencies. Caregivers should work closely with their health care providers to ensure appropriate calories, vitamins, and nutrients are maintained. In some situations, specialized formula taken either orally or via a feeding tube may be recommended to ensure your child receives adequate nutrition.
How does EGID impact an individual's quality of life?
Many individuals with EGID carry on normal daily activities. Some patients, however, experience symptoms that may interfere with school or work. Highly restricted diets can limit participation in social activities that involve food which in turn can create feelings of social isolation. Specialized foods and elemental formulas, missed time from work, associated health care costs, and, in some cases, travel for care is costly and can create a financial strain.
How do environmental/aeroallergens impact patients with EGID?
Patients with EGID commonly have other allergic diseases such as rhinitis, asthma, and/or eczema, so the patient population as a whole generally has an increased sensitivity to both food and environmental allergens. With that said, the relationship between environment allergens and increased EGID symptoms is not clearly understood. Some studies have indicated seasonal variance in the diagnosis of EoE (ie, increased diagnoses during spring, summer, and fall months).
Are there other rare diseases that coexist with EGIDs?
- Yes, EGIDs are associated with several other rare diseases.
- These include but are not limited to the following:
- Hypereosinophilic syndromes (HES)
- Netherton syndrome
- Common variable immunodeficiency (CVID)
- Hyper IgE syndrome
- SAM: Severe dermatitis, multiple allergies, and metabolic wasting syndrome
- Connective tissue disorders (eg, Loeys Dietz syndrome)
- PTEN hamartoma tumor syndrome
- Some of these conditions may compromise the barrier function of the lining of the esophagus or predispose to eosinophilic inflammation.
Can EGID's progress into Hypereosinophilic Syndrome (HES) or Eosinophilic Granulomatosis with Polyangitis (EGPA)?
- Progression of EGID to hypereosinophilic syndrome (HES) or eosinophilic granulomatosis with polyangiitis (EGPA) is rare but has been reported.
- Patients with eosinophilic gastritis/gastroenteritis and blood eosinophil counts ≥ 1,500 may be at increased risk for eosinophilic inflammation in other organs.
Is someone with MCAS more likely to have EGIDs and do the two relate?
- Mast cell activation syndrome (MCAS) is generally diagnosed by:
- Rapid-onset symptoms involving multiple organ systems.
- A favorable response to antihistamines or mast cell stabilizing medications.
- Laboratory evidence of mast cell involvement.
- MCAS may be more common in individuals with autonomic dysfunction and hypermobility.
- There is limited evidence suggesting patients with connective tissue diseases, autonomic dysfunction, and hypermobility may be more likely to have EGIDs.
- More research is needed to determine the meaning of elevated mast cell numbers, shape, and location within the gastrointestinal tract.
Is there a connection between EGIDs, dysautonomia, and connective tissue disease?
- Dysautonomia (also called “autonomic dysfunction”): occurs when the autonomic nervous system is not able to regulate itself properly. The autonomic nervous system is part of the nervous system that controls things that are not usually in our control (eg, heart rate, breathing, and digestion).
- Postural Orthostatic Tachycardia syndrome (“POTS”): a common form of dysautonomia.
- Connective Tissue Diseases: are a group of diseases that affect parts of the body that hold structures together (eg, ligaments, skin, blood vessels, etc.).
- While there are only a few studies on this subject, there does seem to be a link between all these diseases.
- People with EGIDS are more likely to have dysautonomia and connective tissue diseases (particularly women), but we don’t know why yet.
- Treatment of EGIDs does not seem to improve dysautonomia or connective tissue disease.
Is there a link between EGIDs and headaches?
- We don’t know of a link between EGIDs and headaches.
- Headaches are common. Migraine headaches may be more common in other allergic diseases (asthma and allergic rhinitis).
- More research is needed to directly address this question.
What causes esophageal ulcers? How common are they in patients with EoE?
- Esophageal ulcers are most often caused by severe reflux.
- Patients with ulcers usually have more pain with swallowing.
- Ulcerations are not a typical endoscopic feature of EoE but can be seen:
- After a food impaction or dilation procedure.
- If a pill gets stuck in the esophagus and erodes the lining of the esophagus (pill esophagitis).
- In rare cases of esophageal infection (eg, candida, herpes simplex virus (HSV), cytomegalovirus (CMV), HIV, histoplasmosis, and tuberculosis).
- Treatment should be focused on the source of the ulcer.
Eosinophilic Esophagitis (EoE)
Are there different types of EoE and how do they differ?
Yes. Eosinophilic esophagitis (EoE) is a heterogeneous disease and can vary in clinical presentation, endoscopic appearance, response to therapy, and underlying molecular features. Research studies have identified distinct clinical phenotypes, such as inflammatory-predominant and fibrostenotic disease, as well as molecular endotypes based on gene expression patterns within esophageal tissue. These endotypes reflect differences in immune activation, epithelial barrier function, and tissue remodeling. At present, these classifications are primarily used for research purposes. Although they help improve understanding of disease mechanisms, they do not yet reliably predict treatment response or long-term disease course, and EoE management continues to be guided by symptoms, histology, and shared decision-making.
Why are some active EoE patients asymptomatic while others are symptomatic?
- When the esophagus doesn’t function normally it can cause difficulty swallowing.
- Many patients mask the symptoms of EoE with the following adaptive behaviors:
- Drinking liquids to help swallow.
- Cutting foods into small pieces, puree foods.
- Avoiding hard textures.
- Eating slowly.
- Chewing excessively.
- Some patients can have eosinophilic inflammation in the esophagus without symptoms.
- More research is needed to determine if truly asymptomatic patients with eosinophils in the esophagus have a distinct disease or an early form of EoE.
Why is EoE treatment for children different than adults?
- Although most EoE treatments for children and adults should be the same, differences may stem from several factors:
- Adults usually present with difficulty swallowing while children often present with less-specific symptoms including vomiting, abdominal pain, and poor weight gain.
- Adults are more likely to have strictures or narrowing of the esophagus; therefore, esophageal dilation is performed more frequently in adults.
- Treatments (eg, food elimination diets, topical steroids) may be perceived differently in the context of growth, nutrition, and chronicity of disease.
- Families may have more stress and concern about repeated anesthesia and endoscopies in children.
- Some medications are currently only approved for teens and adults (eg, dupilumab).
If I have EoE, are my family members at risk of developing EoE too?
- The overall prevalence of EoE in the general population is low (approximately 0.06%).
- Individuals with an immediate family member (parent/child, sibling) with EoE are at increased risk of EoE compared to the general population, but the risk is modest based on existing studies.
- The increased risk of developing EoE in families is due to both genetic and environmental factors (lack of breastfeeding, geographic location, infections, absence of pets, etc.).
- Additional studies are needed to understand how genetic and environmental factors combine to increase the risk of developing EoE in families.
If IL-5 has been linked to EoE, will there be recommendations for genetic testing specifically for it?
- Interleukin-5 (IL-5) is a biologically relevant protein which contributes to EoE that been targeted for treatment.
- Currently, there is no evidence that variation in the IL5 gene contributes to EoE.
- Given the complex regulatory network driving IL5 expression, it is possible that we are not looking for the variation in the right place.
- Right now, there is not clinical genetic testing for EoE - but that could change in the future.
What role does mold exposure play in EoE?
- There is very little evidence to suggest that mold plays any role in EoE in patients.
- Some researchers have used the mold Aspergillus fumigatus to model EoE in mice.
- White blood cells isolated from patients with EoE may produce more of the cytokine IL-5 in response to stimulation with Aspergillus.
- The rate of EoE diagnosis does not increase with increased mold counts in the air.
- Some patients who are allergic to mold may be more difficult to treat.
- More studies are needed to determine the role of mold exposure in EoE.
Do you believe glutathione deficiencies play a role in EoE?
- We don’t know if glutathione deficiency plays a role in EoE.
- We do know the following about glutathione:
- Glutathione is an important anti-oxidant.
- Glutathione deficiency may be associated with increased inflammation in inflammatory bowel disease (IBD).
- Glutathione deficiency is associated with an increased risk for cancer.
- In contrast, glutathione may be necessary to produce leukotrienes (inflammatory molecule) in EoE.
Does maternal antibiotic exposure cause food allergies and EoE?
- We aren’t sure if maternal antibiotics cause food allergies and EoE.
- A new study suggests that a baby’s risk for EoE may increase the more an expectant mother takes antibiotics.
- The risk for EoE appears to increase the closer the antibiotic exposure occurs to the time of delivery.
- Other risk factors for EoE include:
- Infant antibiotic exposure
- Cesarean delivery Antacid use
Can EoE cause chronic fatigue even when it is in remission?
- Fatigue is common in individuals with EoE.
- The underlying mechanisms connecting fatigue and EoE are unclear; however, patients with EoE may be at risk for nutritional deficiencies, medication side effects, and sleep disruption.
- Patients with EoE may also experience feelings of depression, anxiety, and isolation, which can contribute to fatigue.
- There is limited data on fatigue in well-controlled EoE.
Can EoE cause speech delay?
- We don’t know of any associations between EoE and speech delay.
- Speech delay can be diagnosed alone or caused by something else (eg, hearing loss, autism, intellectual disability).
- Patients with autism are more likely to have EoE.
If someone has EoE and asthma, does it mean they have eosinophilic asthma?
- Not necessarily as there are multiple different subtypes of asthma and EoE.
- Eosinophilic asthma is a subtype of asthma that may be more severe and harder to treat. It can be diagnosed by a lung biopsy, fluid or mucus from the lungs, blood eosinophil counts, or a breath test (FeNO).
- In patients with EoE and other allergic diseases, the risk for eosinophilic asthma is likely increased because both arise from a shared pathophysiology.
- Patients with EoE may have more severe asthma (more persistent with decreased lung function).
- Conversely, patients with asthma may have more severe EoE based on eosinophil counts in the esophagus.
- Treatment approaches for eosinophilic asthma are likely to complement one another and treating one condition is likely to benefit/improve the other.
- Systemic biologics targeting allergic inflammation (IL-4, IL-5, IL-13) may improve both diseases simultaneously.
What is the risk of EoE developing into Barrett esophagus or cancer of the esophagus?
Currently, there is no evidence indicating a link between EoE and esophageal cancer. With that said, patients with EoE often present with reflux/GERD. It is known that, over time, stomach acid in the esophagus can lead to cell changes that increases risk for cancer.
Is it possible to biopsy tissue from an EoE patient's esophagus, grow that tissue in a lab setting and then test it for eosinophilic triggers?
- Yes, there are model systems in place to study the esophagus in the laboratory setting. It may be possible to use these systems to determine food triggers in the future.
- The esophagus is a complex organ supplied by a series of blood vessels that has multiple layers (eg, mucosa, submucosa, muscle, and connective tissue).
- Responses to triggers foods are determined by interactions between esophageal cells and immune cells within the esophagus and the lymph nodes.
- There are several types of models we use to study EoE in the lab:
- In vitro (in test tube/petri dish) – submerged esophageal cell cultures, air-liquid interface cell cultures.
- In vivo (in living body) – animal models.
- Ex vivo (outside living body)– esophageal tissue removed (eg, biopsy, explant) and grown in the lab.
- Organoids (organs in petri dish) – 3-D culture systems that recreate multiple layers of the esophagus.
What is the best treatment for EoE that provides the best quality of life for patients?
- There are several effective medications and dietary treatments for EoE.
- There is not a single ideal therapy that guarantees the best quality of life for all patients.
- Defining the “best” treatment may depend on several medical and non-medical factors.
- The views, lifestyles, preferences of patients are individual, may change, and may differ from those of healthcare providers.
- Recognizing and addressing patient priorities and engaging in shared decision making is crucial to successful management of EoE.
What treatment guidelines exist for women with EoE in pregnancy?
- Limited studies suggest the risk to a mother and her baby is not increased in pregnant women on or off EoE-specific medications.
- Limited studies suggest that EoE symptoms may improve (56%), worsen (20%), or stay the same (24%) during pregnancy.
- Changes in EoE symptoms revert to pre-pregnancy levels in most patients.
- EoE medications considered safe in pregnancy include swallowed topical corticosteroids (budesonide) and proton pump inhibitors.
- Diet elimination during pregnancy is best co-managed with a dietitian with experience in EoE to ensure adequate nutrition.
- Management of EoE during pregnancy should be individualized using a shared decision-making approach between the patient and her physicians.
- Patients with active disease at the beginning of pregnancy may continue treatment.
- Patients with inactive disease may continue treatment or consider stopping treatment with close monitoring.
- Future studies are needed to answer questions about EoE management in pregnancy.
Are EoE and infections related?
- Infections and early-life antibiotic exposure may increase the risk of developing EoE.
- The presence of the bacteria H. pylori in the stomach is associated with decreased identification of EoE.
- Some patients are diagnosed with EoE after herpes simplex virus infections in the esophagus.
- Tick-borne infections (eg, Lyme disease) have not been associated with developing EoE.
- Additional studies are needed to understand whether infections, lifestyle changes, and/or environmental exposures (eg, antibiotics) may contribute to developing EGIDs.
What is the relationship between oral immunotherapy and EoE?
- Oral immunotherapy (OIT) is a new treatment for immediate food allergies.
- OIT dosing begins with a very small amount of the food protein, which is gradually increased over time until a maintenance dose is reached.
- For most patients, OIT must be continued daily to maintain desensitization.
- Patients should discuss the risk of developing EoE during OIT with their provider and should be screened for gastrointestinal symptoms before starting OIT.
- Approximately 5% of patients are diagnosed with EoE during OIT.
- EoE may occur at any time during OIT.
- Some patients may have EoE before starting OIT.
- Usually, EoE resolves after stopping OIT.
- Sublingual immunotherapy (SLIT) for environmental allergies may also cause EoE.
- We do not know why OIT or SLIT causes EoE in some patients.
- New treatments for immediate food allergies are being developed that have not been associated with the development of EoE.
- Patients who experience symptoms of EoE during OIT should discuss whether to continue OIT with their allergist and consider evaluation by a gastroenterologist.
What are the effects of dupilumab on mast cells in patients with EoE?
- Dupilumab is a medication that treats patients with EoE by interrupting one of the ways that may cause problems.
- Dupilumab binds to a very specific protein ( IL-4 receptor alpha (IL-4r𝛼 ) that is known to be linked to EoE.
- This protein is also located on mast cells and stimulating it, may cause mast cells to increase in number and last longer in the tissue.
- Patients with EoE have increased numbers of mast cells in the esophagus and these mast cells may have increased amounts of the IL-4r𝛼.
- Other allergic diseases, such as chronic sinusitis with nasal polyps, have increased numbers of mast cells in the affected tissues.
- Dupilumab decreases mast cells in these diseases; and, thus, may decrease mast cells in the esophageal tissues affected by EoE.
- Additional studies are needed to investigate whether possible effects of dupilumab on mast cells may improve EoE treatment.
Do food triggers of EoE change over time?
- More research is needed to know if food triggers for EoE change over time.
- Persistent inflammation in the esophagus may change the way our immune system recognizes food proteins.
- There are no tests that directly identify EoE food triggers.
- We indirectly identify food triggers in EoE by eliminating food(s) from the diet and repeating biopsies of the esophagus.
- This process can be confusing because sometimes a food trigger is not completely removed from the diet or airborne allergens, like pollens, can also trigger EoE.
- Cross reactivity within and across food groups may be why some patients develop new food triggers.
Why would someone develop EoE if no one else in their family has the disease?
- EoE results from the “perfect storm” of chance combined with genetic and environmental factors [e.g., pollution, infections, medications (antibiotics and antacids), chemicals, cesarean delivery, lack of breastfeeding or lack of furry pets].
- To date, no single factor has been shown to cause EoE by itself.
- Many patients carry genes they pass on to their children that increase disease risk but may not result in disease.
- More research is needed to see if we can predict who will develop EoE.
Should someone with EoE and autoimmune disease be seen by a gastroenterologist and an immunologist?
- Autoimmune diseases are classically defined as harmful immune reactions directed against our own bodies.
- EoE is not considered an autoimmune disease because the immune reactions causing inflammation are directed against food or environmental allergens.
- Patients with EoE are at increased risk for autoimmune diseases.
- These may include autoimmune diseases of the gastrointestinal tract (e.g., celiac disease, inflammatory bowel disease) but also rheumatologic and neurologic diseases.
- Often patients with EoE benefit from treatment by a gastroenterologist and an allergist/immunologist.
- Additional specialists (e.g., rheumatologist, neurologist) may be helpful depending on clinical signs, symptoms, or other medical diagnoses.
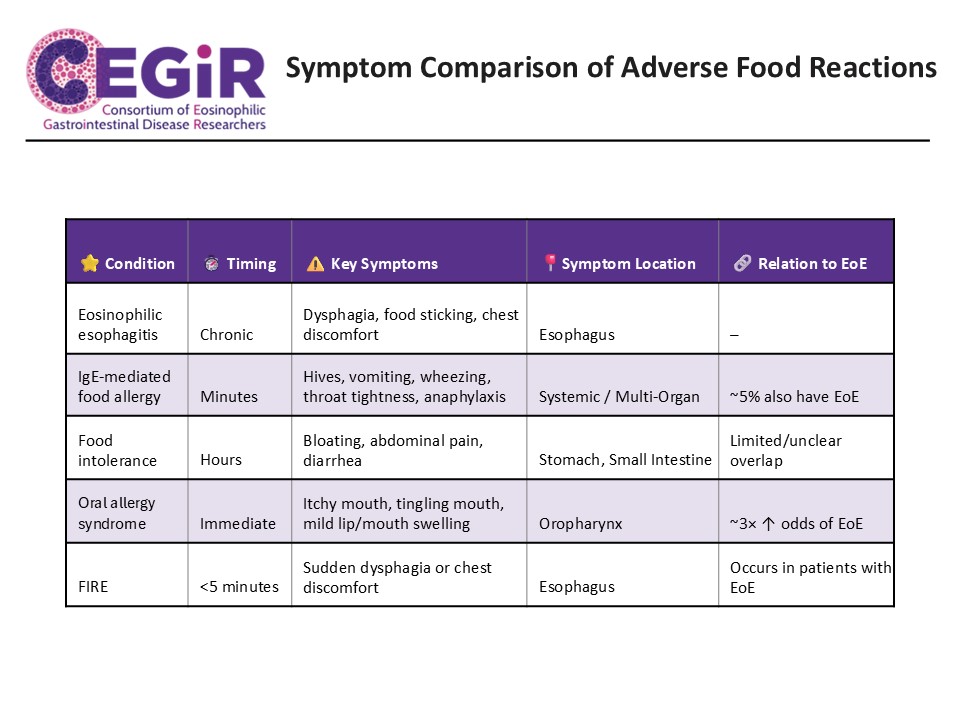
How can we distinguish EoE symptoms from other adverse food reactions?
- EoE symptoms are often delayed and can differ in children (poor weight gain, feeding issues, vomiting, and abdominal pain) and adults (difficulty swallowing, food impaction, and chest discomfort).
- Patients with EoE may also experience symptoms related to other adverse food reactions including IgE-mediated food allergy, food intolerance, oral allergy syndrome (OAS), and food-induced immediate response of the esophagus (FIRE),
- Symptoms associated with these adverse food reactions are listed below:
- IgE-mediated food allergy: hives, swelling, shortness of breath, wheezing, vomiting, throat swelling, or anaphylactic shock usually occurring within minutes of eating a food.
- Food intolerance: abdominal pain, bloating, diarrhea, or vomiting occurring usually occurring within hours of eating a food.
- Oral allergy syndrome (OAS): itching and mild swelling mouth, lips, or throat occurring within minutes of eating a food.
- Food-induced immediate response of the esophagus (FIRE): sensation of burning, pressure or pain in the chest that occurs in a subset of patients with EoE occurring within 5 minutes of eating a food.
Eosinophilic Colitis (EoC)
What causes eosinophilic colitis? Is it autoimmune or caused by foods?
- We do not know the cause of eosinophilic colitis (EoC).
- EoC is an inflammatory disease characterized by the presence of eosinophils that presents with abdominal pain and diarrhea.
- It is important to distinguish between different causes of increased eosinophils in the colon.
- Several diseases/exposures can increase eosinophils in the colon (eg, allergies, medications, infections, autoimmune and connective tissue disorders, hypereosinophilic syndromes and graft vs. host disease).
- In addition to eosinophils, tissue mast cells are increased in EoC.
- Recognition of EoC as a distinct disease category has increased recent efforts to better understand this disease.